
Recurrent tracheoesophageal fistulas (TEFs) may present in 1.9 to 20% of cases after surgical primary closure in patients with esophageal atresia (EA) and TEF.1–3 Respiratory symptoms of chronic cough, episodes of choking and/or cyanosis after eating, recurrent pneumonia, chronic lung disease, and malnutrition should lead to diagnostic suspicion.1,4,5 Upper gastrointestinal series (UGI) and esophagogastroduodenoscopy (EGD) are the diagnostic methods of choice, but repeat studies may be required for confirmation.5 Endoscopic treatment of recurrent TEF has been described as a therapeutic alternative to repeat open chest surgery repair. Some studies have reported on the use of tissue adhesives such as N-butyl-cyanoacrylate (Histoacryl®), fibrin or sclerosing agents, and laser.1–3 We describe herein the case of a preschool child with recurrent TEF managed with a combination of Histoacryl® and lipiodol via esophageal endoscopy.5
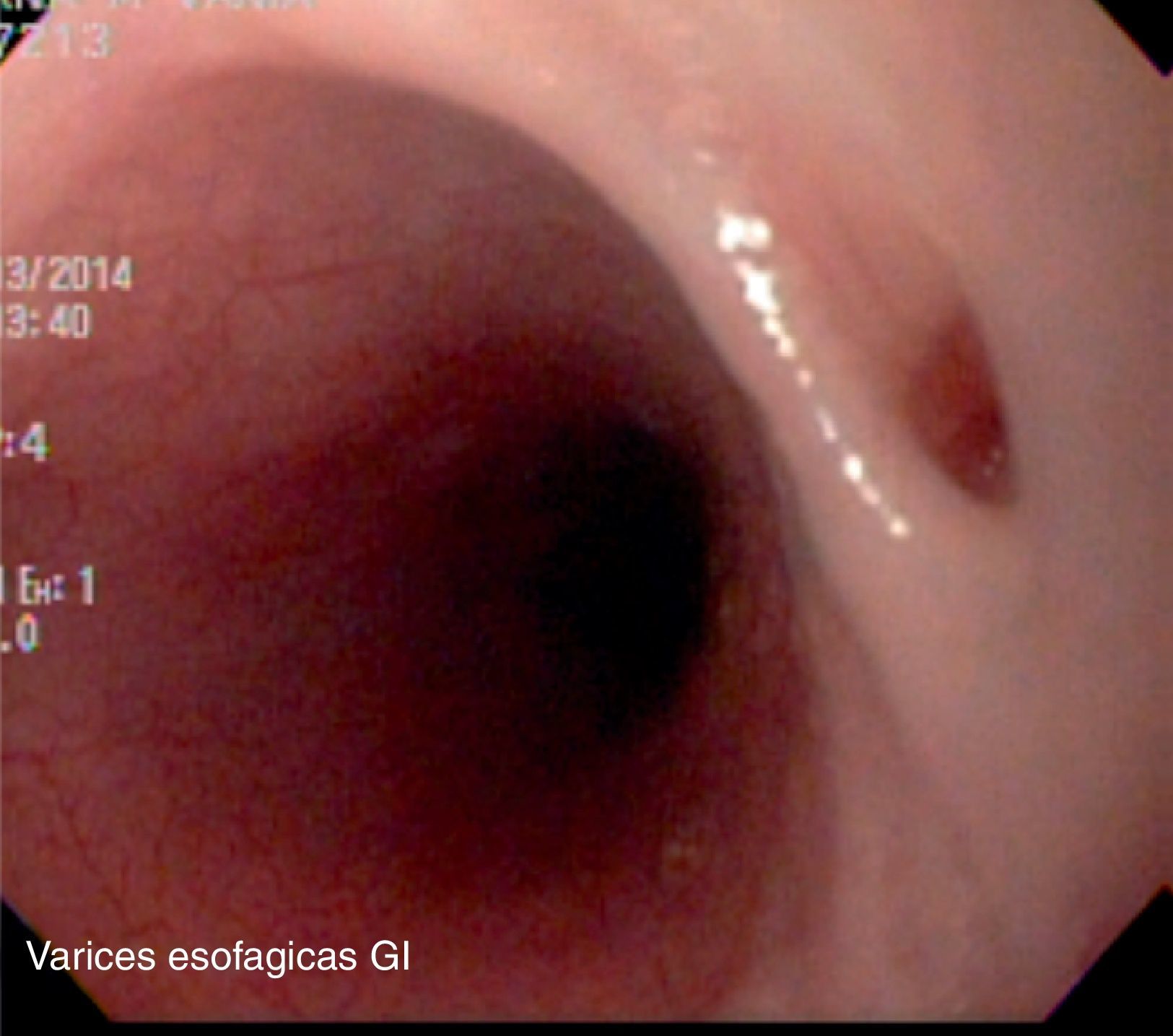
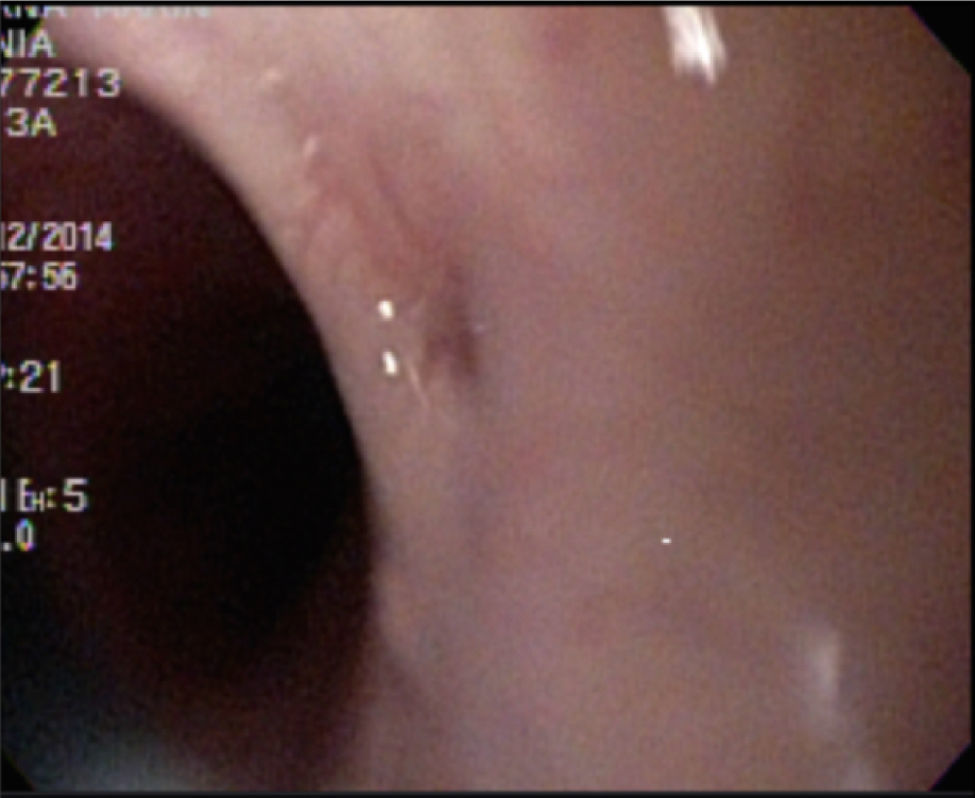
A 3-year-old girl was delivered by cesarean section at 34 weeks of gestation, G2, weighing 1.5kg, and measuring 40cm. She had a past history of severe oligohydramnios, intrauterine growth retardation, and umbilical catheterization. She underwent esophagoplasty at 5 days of life with fistula closure due to type III EA and TEF at another institution. At 19 months of age the patient was referred to the Gastroenterology and Nutrition Service of our hospital because of upper gastrointestinal bleeding causing anemia. She was diagnosed with grade III esophageal varices secondary to portal hypertension and cavernous transformation of the portal vein and was managed with endoscopic variceal band ligation and sclerotherapy with no complications. Starting at 24 months of life, the patient presented with symptoms of repeat pneumonia, gastroesophageal reflux, bronchial hyperreactivity, esophageal candidiasis, pediatric chronic lung disease, and chronic malnutrition, meriting numerous hospitalizations and the use of proton pump inhibitors, inhaled steroids, and short-acting bronchodilators. An EGD was performed when the patient was 3 years old, identifying the TEF opening at 16cm from the incisors and grade II esophageal varices. An esophagogram revealed a short 1.5cm recurrent TEF. Endoscopy with Olympus® GIF-Q150 equipment was programmed, applying a mixture of Histoacryl® (0.5ml) and lipiodol (0.5ml) with an Olympus® sclerotherapy catheter-needle (180cm, 2.3mm) through the opening of the fistula from the distal to the proximal segment without completely covering the edge. There were no reported complications. The quantity of the sclerosing agent was calculated by the size of the fistula as seen in the esophagogram (1.5cm).
With the patient in a fasting state, an esophagogram was carried out 7 days after the procedure with no signs of fistula and an EGD was performed at 15 days. During the 24-month follow-up period there were no new hospitalizations, symptoms of pneumonia, or episodes of choking during eating. The use of bronchodilators and inhaled steroids was reduced and nutritional status improved (Figs. 1 and 2).


The endoscopic treatment of recurrent TEFs utilizing the tissue adhesive Histoacryl® as a therapeutic alternative to surgical reintervention due to its morbidity and mortality was first described in the 1970s.6 Recurrent TEFs may present months or years after surgery, and respiratory symptoms, chronic lung disease, and malnutrition should lead to diagnostic suspicion. There are still few reports of cases in pediatrics and they mainly involve the use of bronchoscopy and a fewer number of esophagoscopies.
Three modalities of endoscopic treatment have been described: 1) injection of tissue adhesive (67% success rate), 2) de-epithelization of the mucosa (14% success rate), and 3) combination of de-epithelization and tissue adhesive (39% success rate).2
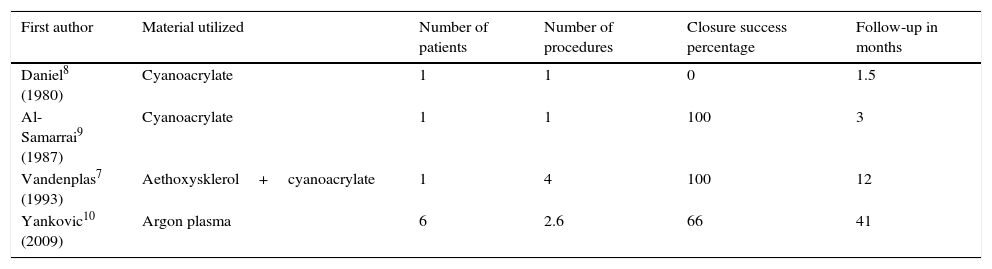
According to reports in the literature, the number of sessions required for achieving successful closure varies from 1 to 4 (Table 1). The use of Histoacryl® via esophagoscopy for recurrent TEF management has been described in pediatrics with a good success rate2 (Table 1).
Endoscopic treatment of the TEF via the esophagus. Success rate and number of sessions. A review of the medical literature.
| First author | Material utilized | Number of patients | Number of procedures | Closure success percentage | Follow-up in months |
|---|---|---|---|---|---|
| Daniel8 (1980) | Cyanoacrylate | 1 | 1 | 0 | 1.5 |
| Al-Samarrai9 (1987) | Cyanoacrylate | 1 | 1 | 100 | 3 |
| Vandenplas7 (1993) | Aethoxysklerol+cyanoacrylate | 1 | 4 | 100 | 12 |
| Yankovic10 (2009) | Argon plasma | 6 | 2.6 | 66 | 41 |
Source: modified table of Meier et al.3
Vandenplas et al. reported on a 12-year-old female patient with TEF managed with a combination of Histoacryl® and Aethoxysklerol®, achieving successful closure in 4 esophagoscopy sessions.7
The success rate of recurrent TEF endoscopic treatment has been reported at 39-48% with a first session and 60-81% with 2 sessions or more.1,3
In the case of our patient, we used a combination of Histoacryl® and lipiodol. The latter is useful for evaluating complications associated with the application of cyanoacrylate, for radiographic control (embolisms and perforations), and for achieving polymerization of the tissue adhesive in 10-12seconds. A single session was performed with no de-epithelization of the edges of the mucosa and no apparent complications at the 24-month follow-up. Associated complications are respiratory difficulty and death in 1.7% of the cases.2
The risk for refistulization after the procedure may present in up to 63% of the cases, requiring 1-6 procedures for successful closure and in some cases a second surgical intervention is necessary. Therefore, patient selection and follow-up are important. Up to the present, our patient has had no fistula recurrence.
The diagnosis of recurrent TEF is a challenge for the attending physician, and by virtue of clinical suspicion, EGD and endoscopy are required for confirming the diagnosis. Endoscopic treatment with tissue adhesives is an option in selected patients presenting with greater morbidity and in whom surgical intervention involves a greater risk.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Cadena-León JF, Quimbayo-Wilches DM, Ramírez-Mayans JA, Cervantes-Bustamante R, Toro-Monjaraz EM. Tratamiento endoscópico de fístula traqueoesofágica recurrente con una combinación de N-butyl-2-cianocrilato (Histoacryl®) y lipiodol por esofagoscopia en pediatría. Revista de Gastroenterología de México. 2016;81:233–235.

