
Introducción: La infección por Helicobacter pylori (Hp) presenta alta prevalencia mundial, asociada a gastritis hasta cáncer gástrico. Informes sugieren que el alcohol tiene acción antibacteriana; su concentración y cantidad de ingesta, disminuyen el riesgo de infección por Hp; en contraste, diversos estudios relacionan el tabaco y el consumo de café como factores de riesgo para infección por Hp, siendo controvertido.
Objetivos: Comparar la frecuencia del consumo de alcohol en pacientes con infección por Hp con aquellos sin infección y secundariamente comparar la asociación de tabaquismo y consumo de café con infección por Hp.
Material y métodos: Estudio de casos y controles realizado en trabajadores del estado de Sinaloa, que fueron sometidos a endoscopia y prueba serológica de Hp. Se definió caso a pacientes con test sérico para Hp o biopsia con prueba rápida de ureasa positivos. El consumo de alcohol se categorizó como: no consumo, bajo riesgo y en riesgo. Muestra: 269 sujetos por grupo. Se estimaron la razón de momios y los intervalos de confianza del 95%.
Resultados: La edad promedio ± desviación estándar de los sujetos fue de 45.7 ± 9 años en ambos grupos (p = 0.99); el género se distribuyó en 139 mujeres (51.7%) y 130 hombres (48.3%); consumo de alcohol 108 (40.1%) y 85 (31.6%) en casos y controles, respectivamente (p = 0.039), RM 1.45 (IC del 95%, 1.019-2.069). La cantidad en gramos de alcohol en sujetos con consumo en riesgo fue significativa; sin embargo, no hubo diferencias significativas en relación con el consumo de tabaco y café entre los grupos.
Conclusiones: Se observó asociación entre el consumo de alcohol y la infección por Hp, sin asociación a tabaquismo y consumo de café.
Introduction: There is a high prevalence worldwide of Helicobacter pylori (Hp) infection associated with gastritis and extends to gastric cancer. Reports have suggested that alcohol has antibacterial action and that its concentration and the amount consumed reduce the risk for Hp infection. In contrast, different studies suggest that tobacco and coffee consumption arerisk factors for Hp infection, but their results are controversial.
Aims: To compare the frequency of alcohol consumption in patients infected by Hp with thatof non-infected subjects and, as a secondary aim, to compare the association of smoking and coffee consumption with Hp infection.
Material and methods: A case-control study was conducted on Sinaloa State workers that underwent endoscopy and the Hp serology test. Cases were defined as patients with a positive Hp serology test or a positive biopsy with the rapid urease test. Alcohol consumption wascategorized as: no consumption, low-risk, and at-risk. The sample included 269 subjects pergroup. Odds ratio (OR) and 95% confidence interval (CI) were calculated.
Results: In both groups, the mean age of the subjects was 45.7 (SD: 9) years (P=.99), 139 of the subjects were women (51.7%) and 130 were men (48.3%); alcohol consumption was present in 108 (40.1%) and 85 (31.6%) of the cases and controls, respectively (P=.039), OR 1.45 (95%CI 1.019-2.069). The quantity of grams of alcohol in subjects with at-risk consumption was significant; However, there were no significant differences in relation to smoking and coffee consumption between the groups.
Conclusions: An association between alcohol consumption and HP infection was observed and no relation with HP infection was found with respect to smoking and coffee consumption.
Introduction
Helicobacter pylori (Hp) is a bacterium that infects the epithelial mucosa of the human stomach. In 1981 Marshall BJ and Warren JR isolated this microorganism and cultivated it from the gastric mucosa, establishing the fact that many gastric ulcers, as well as gastritis, were caused by the colonization of this bacterium in the stomach.1 Infection due to Hp is the most common worldwide and is associated with diseases of the gastrointestinal tract that include chronic gastritis, functional dyspepsia, peptic ulcer disease, and gastric cancer. Epidemiologic evidence indicates that the majority of infections due to Hp are acquired in infancy.2 Its prevalence is associated with socioeconomic conditions and this infection is more common is the developing countries than in developed countries such as the United States,3 where the prevalence of Hp infection is from 30-40%.4 In Mexico prevalence has been reported from 79% in the open population5 to 87% in patients6; the national survey in which serology was the screening method showed Hp infection prevalence to be 66%.7 The Hp infection transmission mechanism is oral-oral or fecal-oral, as well as through contaminated water.8 The pathogenic potential of the circulating Hp strains has been regarded as a decisive factor in infection progression and in the development of gastric cancer,9 and so have the elements of geography and race.10 Some authors in the United Kingdom have described how adult lifestyle factors such as smoking and alcohol consumption could have an influence on the spontaneous eradication of Hp.11 There are reports that suggest that alcohol has antibacterial action and, depending on its concentration and the quantity ingested, reduces the risk for infection through the induction of adaptive cytoprotection as a result of its long-term use, whereas others state that there is no difference in prevalence between alcoholics and the normal population.12 Experimental studies in rats have shown that the intragastric administration of ethanol produces gastric mucosal adaptation. It is associated with greater cellular proliferation and an increase in the mucosal expression of the transforming growth factor-alpha and the epidermal growth factor; this mechanism, however, is still unexplained.13 The data from the 2008 Mexican National Addiction Survey reveal that 8 out of every 1000 persons report consuming alcohol every day, at a proportion of 7.5 men to 1 woman. Beer is the preferred beverage of the Mexican population, followed by distilled alcohols (spirits); table wine and prepared drinks are consumed at a significantly lower proportion. There are almost 4 million habitual drinkers (5 or more drinks for men and 4 or more for women once a week) and the more frequent proportion is 5.8 men to 1 woman.14 Any level of alcohol consumption implies health risks.15 International study designs have made reference to the presence of Hp infection with that of alcohol consumption. The decision to conduct the present study was based on both the prior publications by different researchers and the idea that the lifestyle habits in the Mexican environment in relation to the consumption of alcohol, and secondarily, of coffee and tobacco, are probable risk factors that could change and/or prevent gastric disorders, or to the contrary, might provide still unidentified benefits. The hypothesis was that patients presenting with Hp infections have a lower frequency of alcohol consumption than those with no infection. The aim of the study was to compare the frequency of alcohol consumption in patients with and without Hp infection; and as secondary aims, the association of smoking and coffee consumption with Hp infection in those patients.
Material and methods
An observational, longitudinal, comparative, case-control study was designed. It was approved by the Research and Ethics Committee of the Hospital Regional del Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado in Culiacan, Sinaloa. The population studied was made up of adult patients seen as outpatients of that hospital unit located in the northwest of Mexico within the time frame of January 1, 2010 to August 15, 2011, as well as incidental patients seen from September 1, 2011 to February 15, 2012. Two groups were formed: cases (n = 269) and controls (n = 269). Cases were defined as adult patients with a positive Hp serology test or a positive biopsy with the rapid urease test, and controls were defined as adult patients with a negative Hp serology test or a negative biopsy with the rapid urease test. The selection criteria were: adult patients between the ages of 25 and 60 years, of either sex, State workers, natives of the State of Sinaloa, and patients that signed statements of informed consent. The exclusion criteria were: patients with a past medical history of gastric surgery, recent ingestion of proton pump inhibitors (2 weeks prior to the study), antibiotics and bismuth salts (4 weeks prior), and patients previously treated for Hp infection. The elimination criteria were: errors in the laboratory results due to poor Hp test technique.
The study subjects underwent endoscopy for the following reasons: dyspepsia with alarm symptoms (digestive tract bleeding, unintentional weight loss), organic pathology (duodenal ulcer cicatrization control), gastroesophageal reflux disease under certain circumstances such as esophagitis, for Barrett's esophagus control, and for dyspepsia under investigation.
The independent variable was Hp infection and the dependent variable was alcohol consumption.
Operationalization of the variables. Hp infection. Based on the rapid chromatographic immunoassay test using the Hp Fast kit (GI Supply, Chek-Med Systems, Inc. PA, USA), the qualitative detection of the Hp antibodies IgG, IgA, and IgM in human serum and/or endoscopic biopsy with the rapid urease test were carried out. The serology test was negative (absence of Hp infection) when only a single violet control line appeared in the upper part of the window, and positive (presence of Hp infection) when there was a change in the pH indicator color, from yellow to fuchsia, within the time frame of minutes to a maximum of 1 h.
Alcohol consumption. It was defined according to the United States National Institute on Alcohol Abuse and Alcoholism16 (NIA A A) and the Dietary Guidelines for Americans from the U.S. Department of Agriculture and Department of Health and Human Services17,18 as:
— Low-risk alcohol consumption: up to 1 drink per day and not more than 7 drinks per week for women and up to 2 drinks per day and not more than 14 drinks per week for men.
— At-risk alcohol consumption: more than 3 drinks per day or more than 7 drinks per week for women and more than 4 drinks per day or more than 14 drinks per week for men.
— No alcohol consumption: absolutely no consumption of alcoholic beverages for men and women.
A "standard" drink was defined as 12 fluid ounces of regular beer (5% alcohol), 5 fluid ounces of wine (12% alcohol), or 1.5 fluid ounces of 80-proof spirits (40% alcohol). Standard drinks contain 0.6 ounces (16 grams) of pure alcohol.
Coffee consumption. Those subjects that presently drink 1 or more cups of coffee daily and that have done so for more than one year were considered coffee consumers. Consumption was categorized as: no coffee consumption with 0 cups per day, 1-2 cups per day, and ≥ 3 cups per day.19
Smoking. Subjects were regarded as smokers if they smoked at least 1 cigarette within the last month (whatever quantity). Non-smokers were those that had never smoked or that had smoked fewer than 100 cigarettes during their lives.20 The grade of smoking: the mild smoker was the subject that smoked less than 5 cigarettes per day; the moderate smoker, an average of 6-15 cigarettes per day, and the heavy smoker, an average of more than 16 cigarettes per day.21
Sample size. An n of 269 subjects with an 80% power for detecting a difference between proportion of 0.10 (Delta) was calculated. The proportion in group one (the treatment group) was assumed to be 0.27 under the null hypothesis and 0.37 under the alternative hypothesis. The statistical test used was the unilateral (one-tailed) Z test and the significance level was 0.05.
The sample was random and stratified by sex and age. An observational measuring instrument was used (the Hp infection variable was measured using the serology test for Hp antibodies and the urea-urease rapid test) and the data recollection for alcohol consumption, coffee consumption, and smoking (2 measurements: current consumption and consumption more than one year before) was carried out through the clinical case records and by telephone interview for the prevalent cases and a medical office interview for the incidental cases.
The statistical analysis was done with the SPSS version 16 package (SPSS, Inc., Chicago IL, USA). Means and standard deviation were used for the descriptive statistics for the quantitative variables, and the categorical variables were presented as frequencies and percentages. The mean comparison was made using the Student's t test and the categorical variables were compared using the Pearson chi-square test (univariate). The multivariate backward stepwise logistic regression was used to analyze the relation between the dependent and independent variables. The odds ratio (OR) was calculated with 95% confidence intervals with a p ≤ 0.05.
Results
The cases and the controls had 269 subjects each and the groups were stratified by age and sex; the mean age of the subjects was 45.7 years (SD: 9) in both groups (p = 0.99); and the sex distribution was 139 (51.7%) women and 130 (48.3%) men in both groups (p > 0.05).
In the case group, Hp infection was diagnosed through the Hp serology test in 214 (79.6%) patients and through endoscopy with the rapid urea-urease test in 55 (20.4%) patients. In the control group, diagnosis was made through the Hp serology test in 199 (73.97%) patients and through endoscopy with the rapid urea-urease test in 70 (26.03%) patients.
Indications for endoscopy for the case group were dyspepsia under investigation in 22 (44%) patients, gastroesophageal reflux disease in 16 (32%), dyspepsia with alarm symptoms in 7 (14%), Barrett's esophagus control in 3 (6%), and duodenal ulcer cicatrization control in 2 (4%). Indications for endoscopy in the control group were dyspepsia under investigation in 38 (54.3%) patients, gastroeso phageal reflux disease in 31 (44.3%), and Barrett's esophagus control in 1 (1.4%).
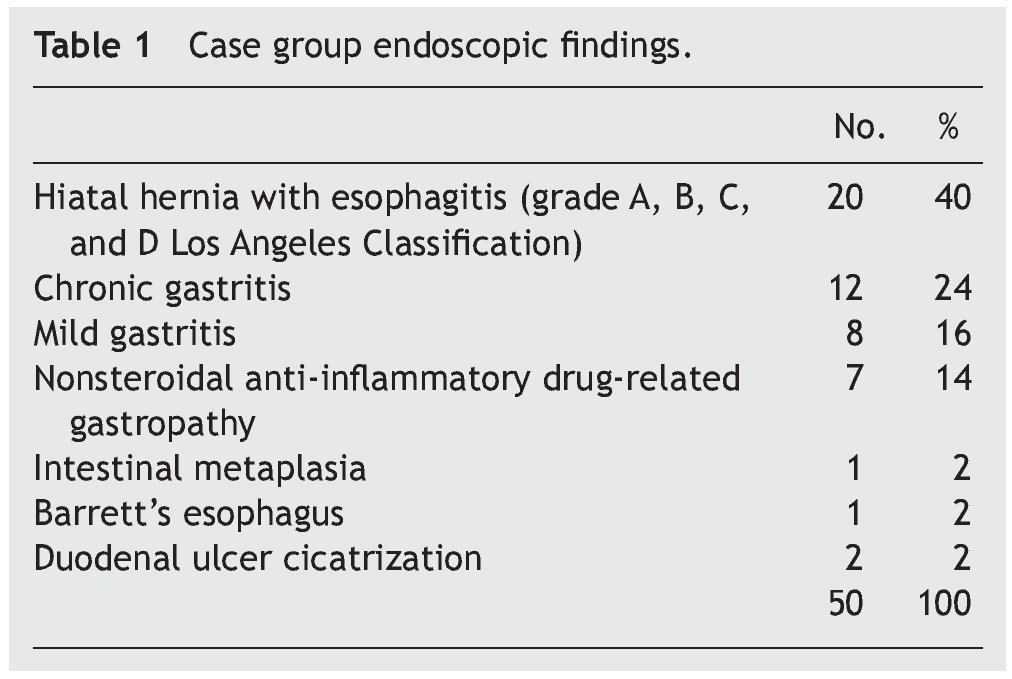
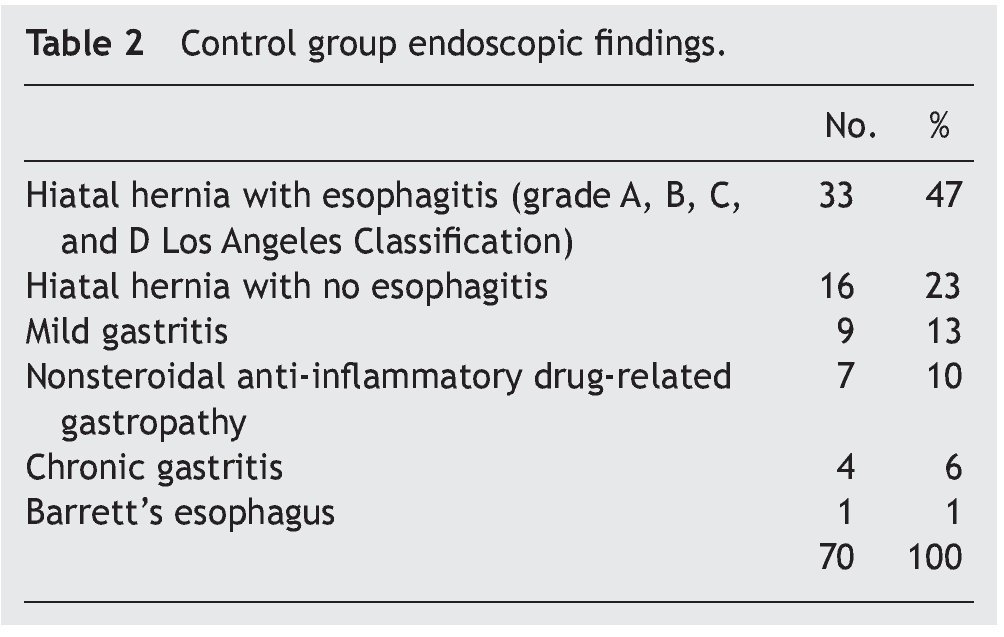
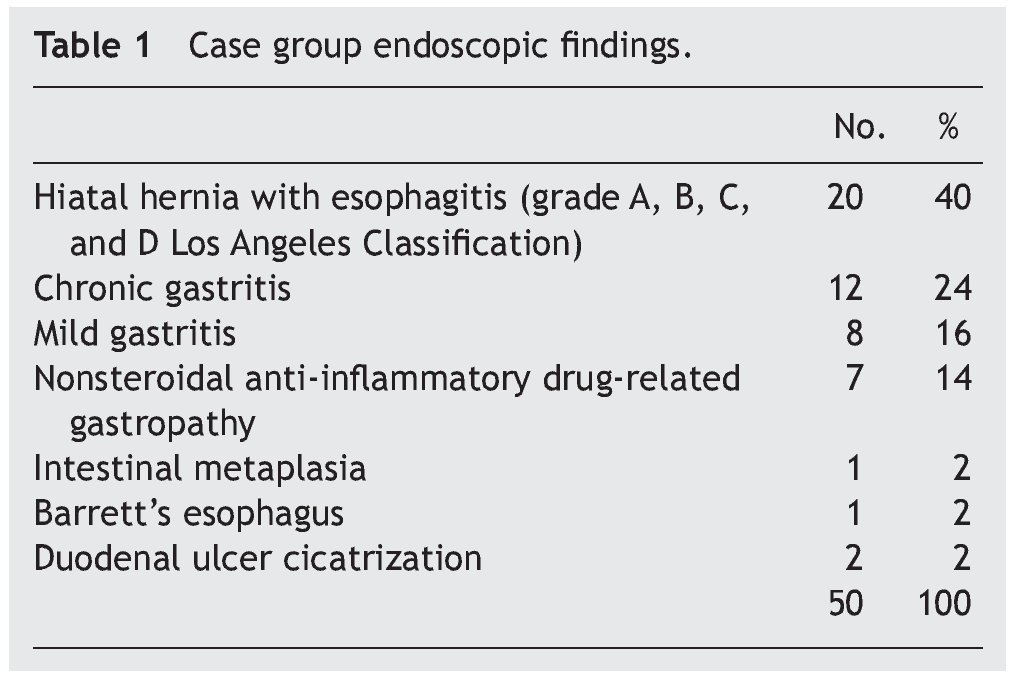
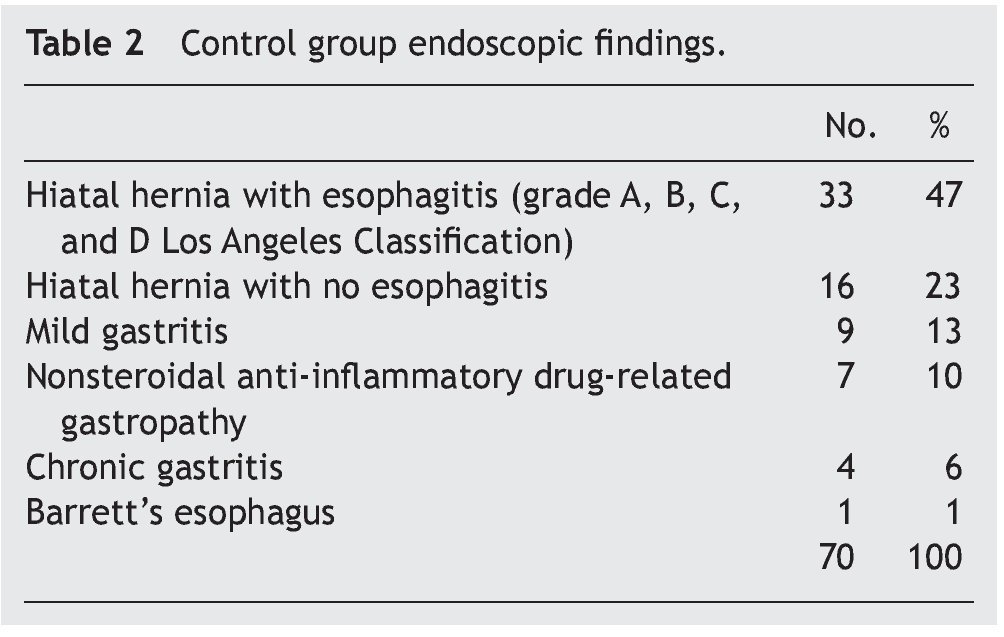
The most frequent endoscopic findings for the case group were hiatal hernia with esophagitis (the Los Angeles Classification grades A, B, C, D) in 20 (40%) patients and chronic gastritis in 12 (24%) (Table 1). For the control group, the most frequent endoscopic findings were hiatal hernia with esophagitis (the Los Angeles Classification grades A, B, C, D) in 33 (47%) patients and hiatal hernia without esophagitis in 16 (23%) (Table 2).
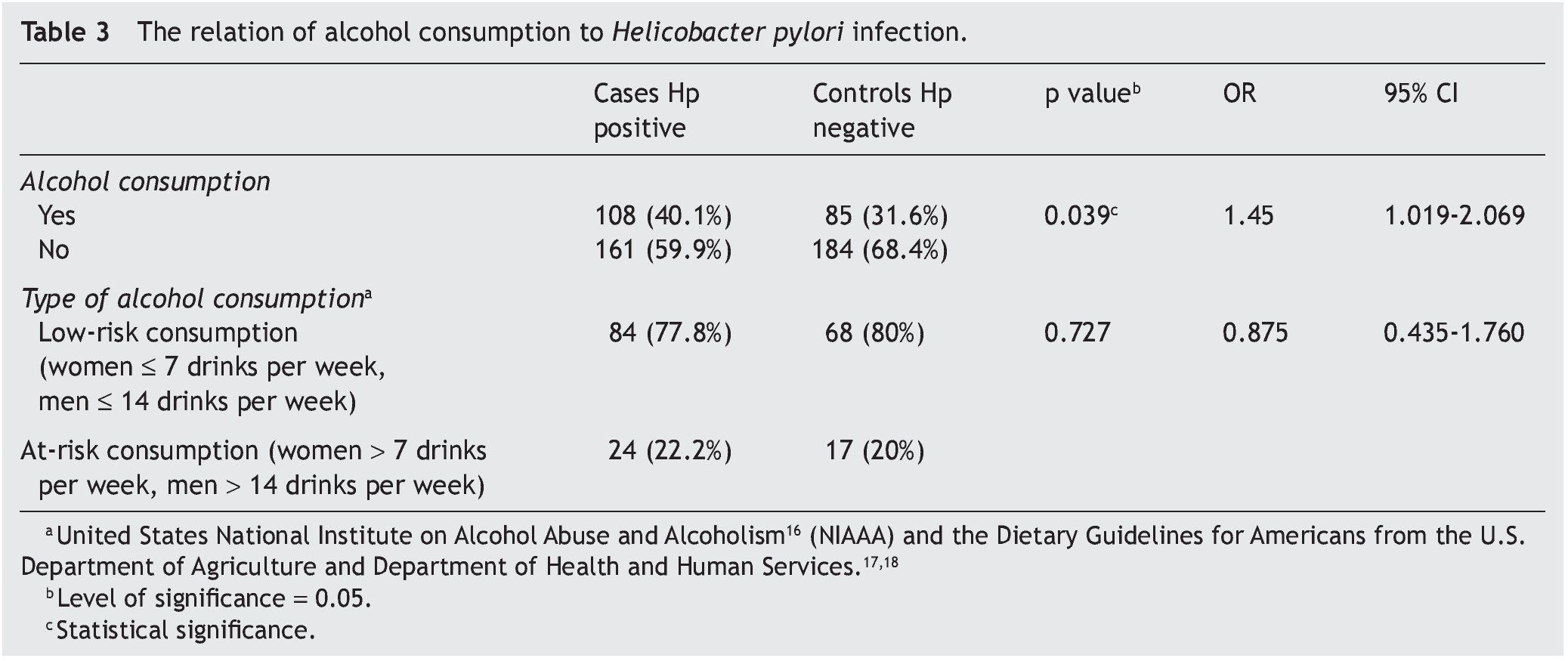
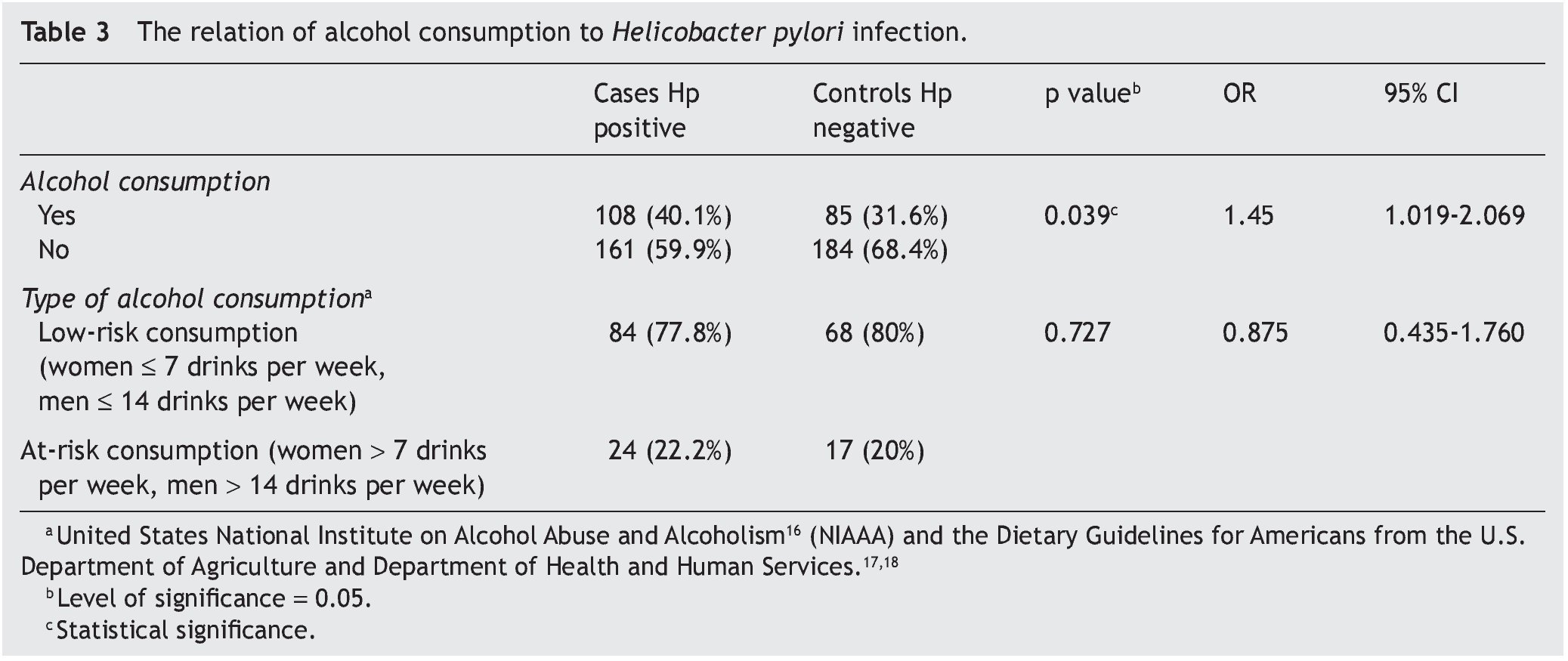
Alcohol consumption was present in 108 (40.1%) and 85 (31.6%) patients in the cases and controls, respectively, (p = 0.039) with an OR of 1.45 (95%CI 1.019-2.069). In reference to the type of alcohol consumption, there was no significant difference between low-risk and at-risk consumption in either group (p = 0.727) (Table 3).
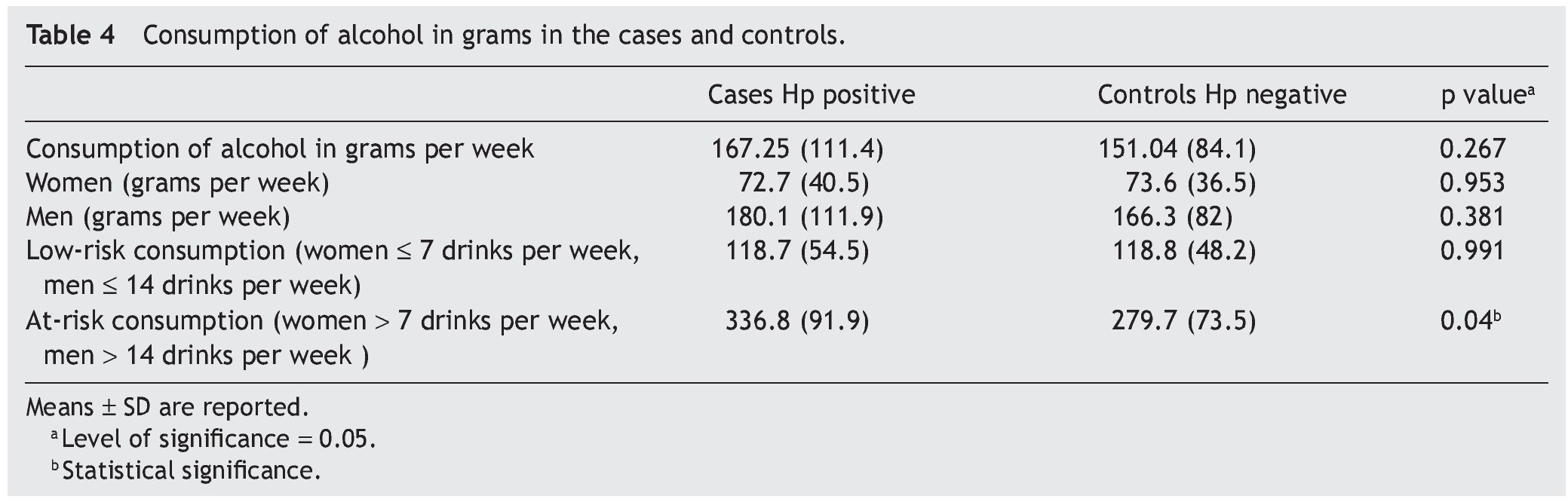
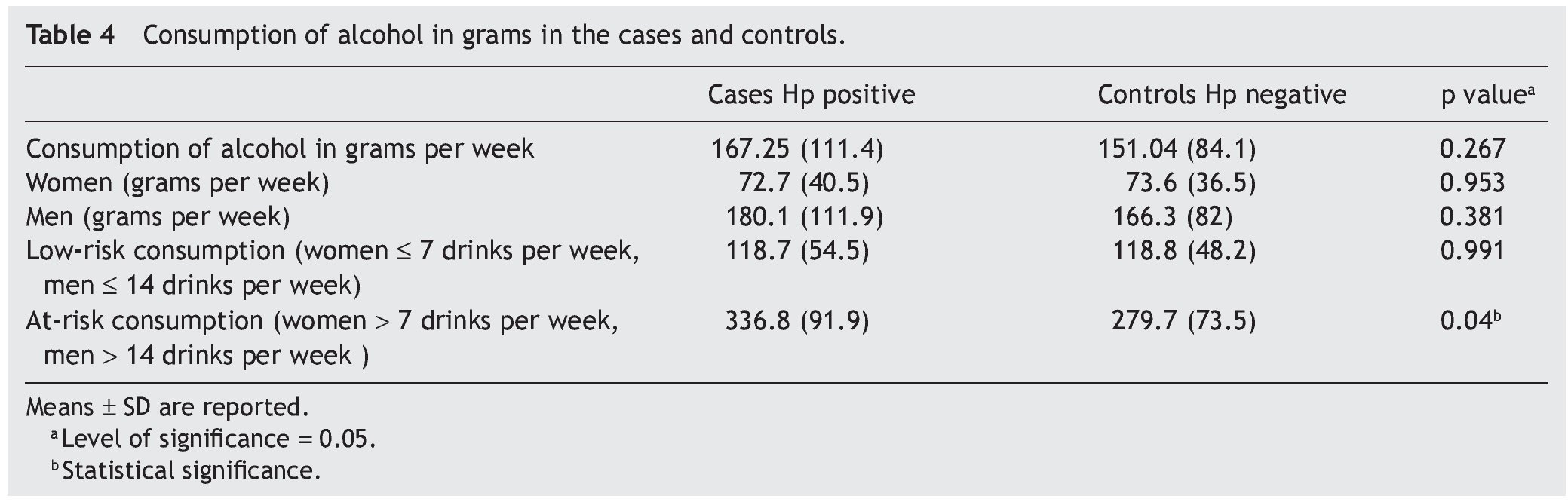
The mean alcohol consumption in grams was 167.25 ± 111.4 in the cases and 151.04 ± 84.1 in the controls, with a p = 0.267; according to the mean alcohol consumption in grams in subjects with low-risk consumption there was no significant difference between the cases and controls (p = 0.991); however, there was a significant difference between the two groups in relation to at-risk consumption (p = 0.04) (Table 4).
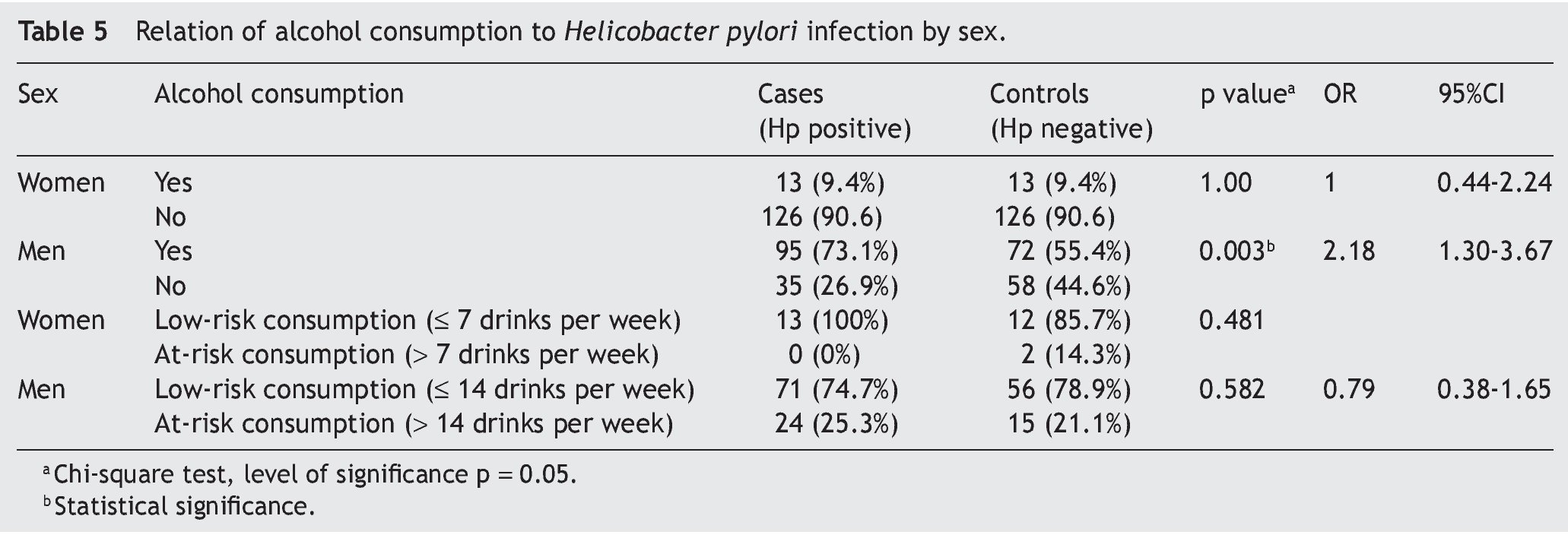
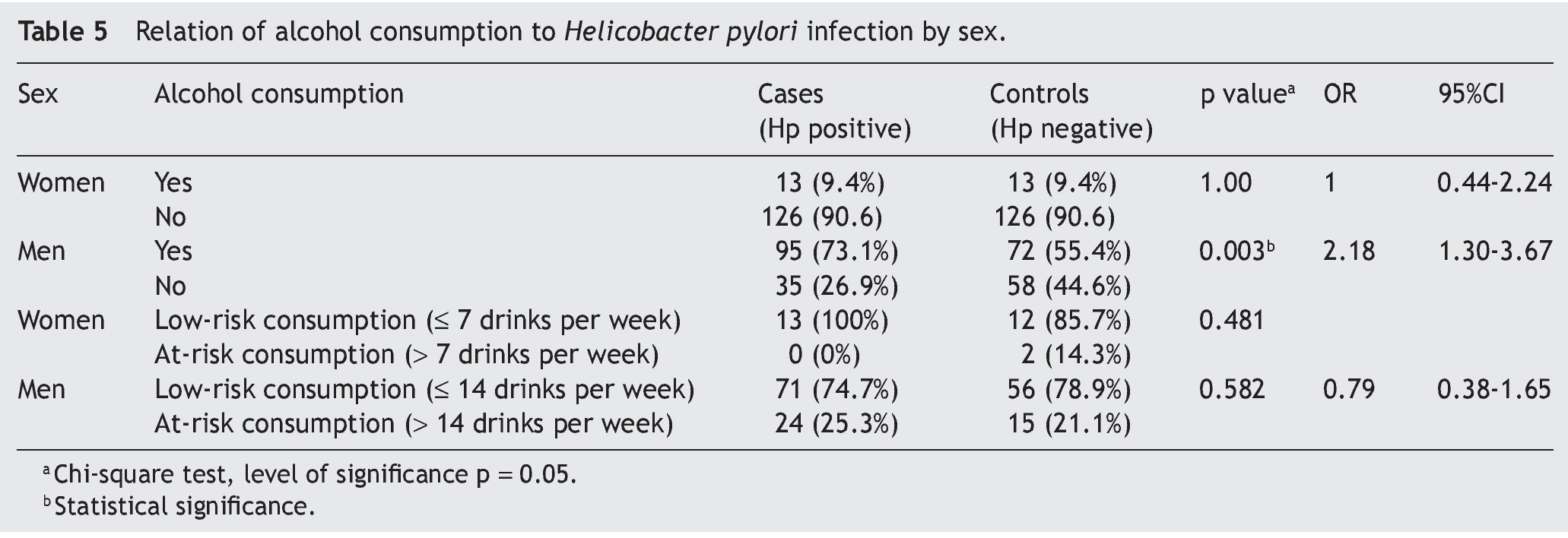
There was an association between Hp infection and alcohol consumption in men (p = 0.003) with an OR of 2.18 (95%CI 1.30-3.67); there was no significant difference in women. No significant difference was observed in the association of Hp infection with low-risk or at-risk consumption in relation to sex (Table 5).
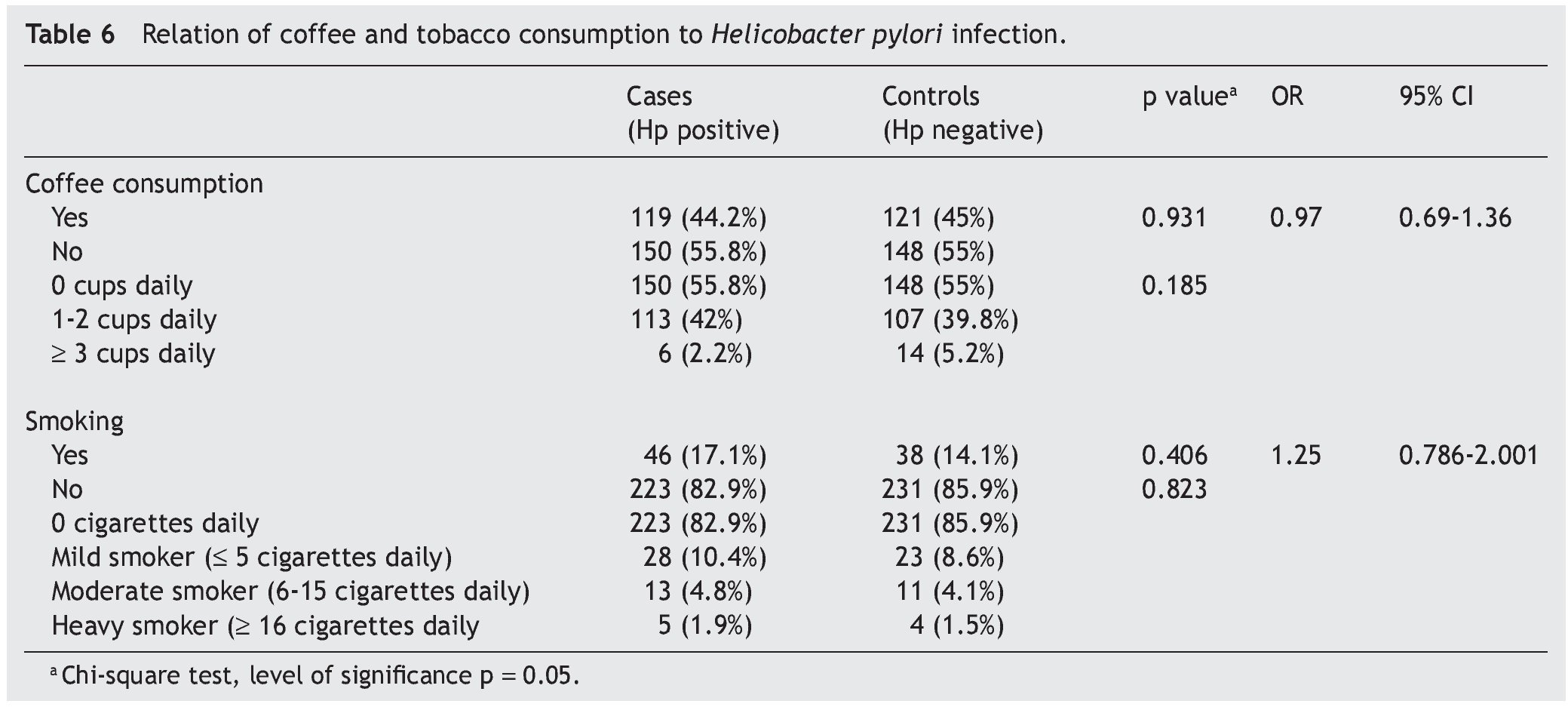
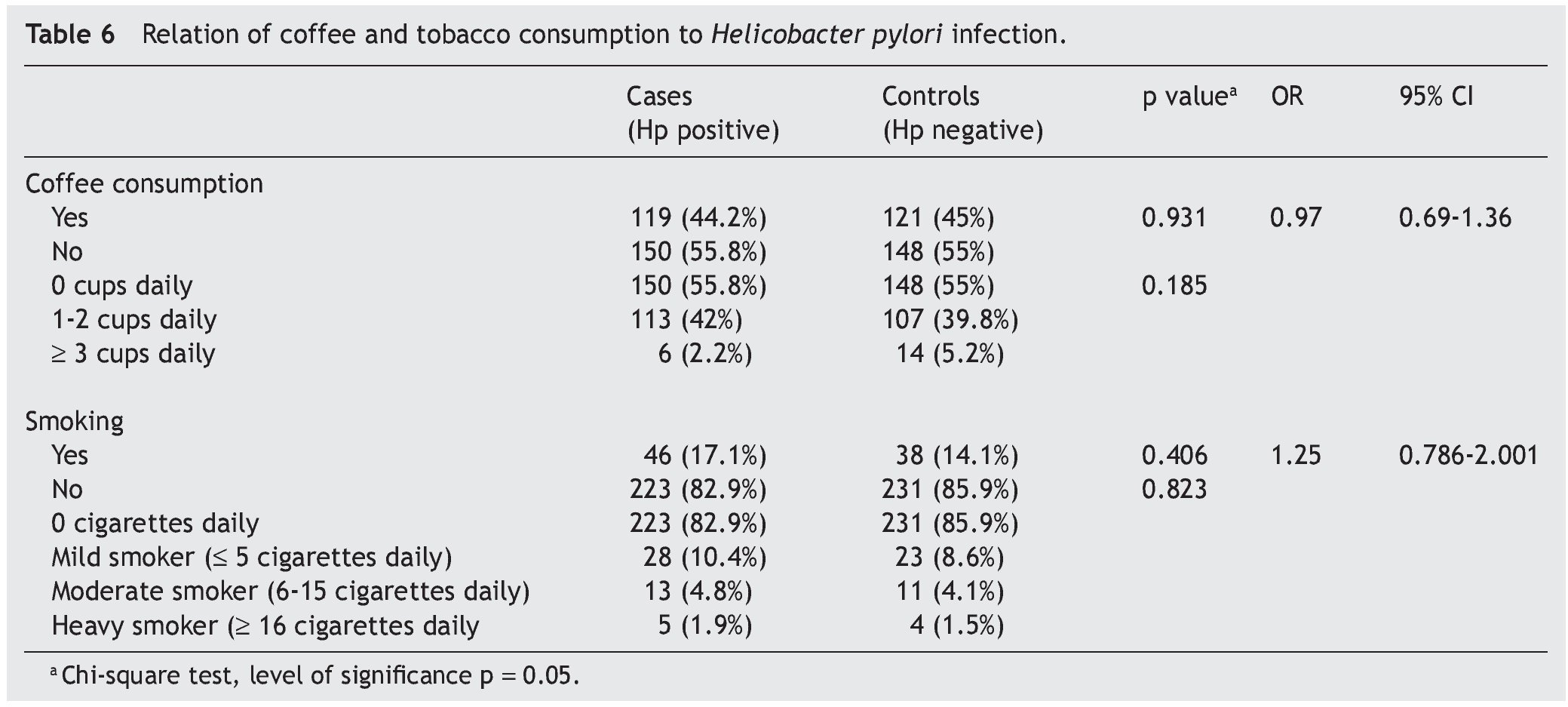
There was no significant difference between Hp infection and coffee consumption and the number of cups ingested, nor was there statistical significance between the 2 groups in relation to smoking or the number of cigarettes smoked daily (Table 6).
In the backward stepwise logistic regression analysis, smoking was eliminated in the first step (p = 0.754), coffee consumption in the second step (p = 0.737) and there was statistical significance (p = 0.039) for alcohol consumption in the third step with an OR of 1.452 (95%CI, 1.019-2.069).
Discussion
The results of the studies related to the association between Hp infection and at-risk alcohol consumption are still controversial, given that some authors found no association between the 2 factors.22-24 Other authors suggest that alcohol consumption has a protective effect against active Hp infection, contrary to that of coffee consumption.25,26 Some results conclude that smoking and alcohol consumption are protective factors against Hp infection.27 There are studies that found no association between Hp infection and alcohol and coffee consumption, but in which smoking was a risk factor.28 Some authors report that moderate alcohol consumption could be inversely associated with Hp seroconversion.19,29 Nevertheless, after studying the relation of factors such as diet and socioeconomic status, it has been supposed that there is no association between Hp infection and alcohol consumption, coffee drinking, or smoking.30
A relation between alcohol consumption and Hp infection was observed in the present study, and the risk for infection was greater in the subjects that consumed alcohol than in those that did not; the risk for infection was up to 1.45 times greater with an interval of 1.01 to 2.06. Men had twice the risk for Hp infection than women, with an interval of 1.3 to 3.6. The quantity of grams per week of at-risk alcohol consumption was greater in individuals with Hp infection than in those without it. Smoking and coffee consumption were not risk factors for Hp infection.
These results differ from those of other authors22,24,28 that found no association between alcohol consumption and Hp infection. In contrast to our results, other researchers11,19,25-27 suggest a protective effect of alcohol consumption in relation to active Hp infection.
Unlike the present study, Brenner H et al.25,26 found that coffee consumption was associated with an increase in the risk for Hp infection. On the other hand, Moayeddi P et al.28 and Gikas A et al.19 found no association with coffee consumption.
In relation to smoking, Ogihara A et al.27 concluded that smoking has a protective effect against Hp infection, whereas Moayeddi P et al.28 stated that smoking was a risk factor. These results are different from those of the present study.
Results of other studies,19,22,24 similar to those of our study, found no association between smoking and Hp infection.
This diversity of results may be related to different conditions between countries (socioeconomic level, environmental atmosphere, biological variability, etc.), as well as to the fact that in scientific studies there are often arbitrary classification ranges and difficulties of adequate measurement control of the variables.
The NIAAA criteria16 point out that alcohol consumption of 4 or more drinks within a 2 h period at least once a week for women and 5 or more drinks for men, referred to as "binge drinking" and regarded as somewhat «risky» drinking, is associated with alcohol dependency. A limitation of the present study is the fact that binge drinking was not evaluated. It should be taken into account in future epidemiologic studies related to alcohol consumption.
Like all case-control designs, this study did not involve time sequence and therefore cannot demonstrate causality. Case-control studies are prone to problems of bias (information quality, memory, case selection, among others) and the possible sources of bias were considered.
In conclusion, the present study showed an association between alcohol consumption and Hp infection. The risk for Hp infection was greater in the subjects that consume alcohol than in those that do not. Likewise, the weekly quantity of grams of at-risk alcohol consumption was greater in the individuals infected with Hp. There was no association with smoking and coffee consumption.
Financial disclosure
Financial support was received from the Universidad Autóno ma de Sinaloa in the Programa de Fortalecimiento y Apoyo a Proyectos de Investigación (PROFAPI-2012).
Conflict of interests
The authors declare that there is no conflict of interest.
Acknowledgments
The authors wish to thank the endoscopy and laboratory personnel of the Hospital Regional del ISSSTECuliacán, as well as the Universidad Autónoma de Sinaloa, for their support.
Received 27 October 2012;
accepted 6 June 2013
* Corresponding author at:
Servicio de Gastroenterología, Hospital Regional Culiacán.
Calzada Heroico Colegio Militar 875 sur, colonia 5 de Mayo, CP 80000, Culiacán, Sinaloa, Mexico.
Tel.: +66 71 59 34 00 Ext. 272.
E-mail address: sanchezcuen jaime@hotmail.com (J.A. Sánchez-Cuén).

