
Sodium bicarbonate ingestion in the general population is common, given that it is an antacid employed for dyspepsia and gastroesophageal reflux, but it has been associated with spontaneous gastric rupture. The first case was reported in 1842 by Thompson et al.1 The phenomenon has not been widely studied, and the following are among the most common causes of spontaneous gastric perforation: abundant food ingestion by patients with psychiatric disorders (anorexia nervosa and bulimia), sodium bicarbonate ingestion, superior mesenteric artery syndrome, gastric infarction, strangulated hiatal hernia, gastric volvulus, and trauma. Because it is a pathology with a high mortality rate, it requires immediate intervention. Thus, emphasizing the existence of these cases is of the utmost importance.2
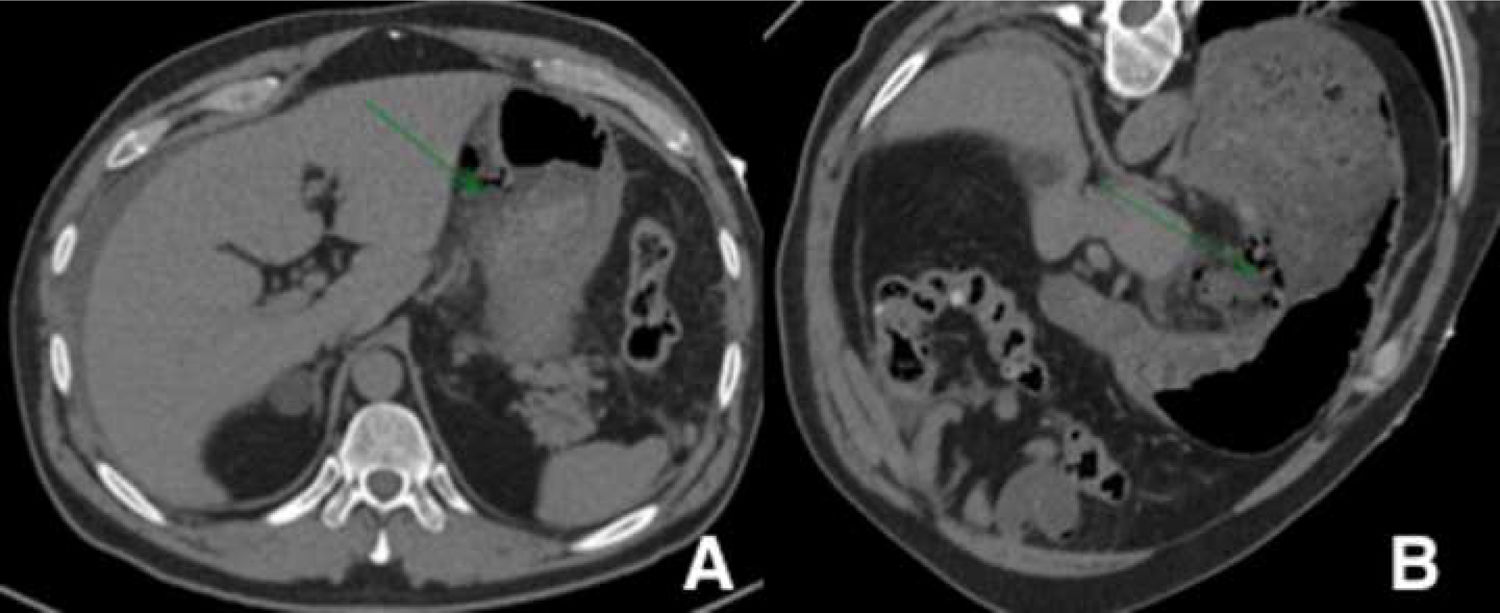
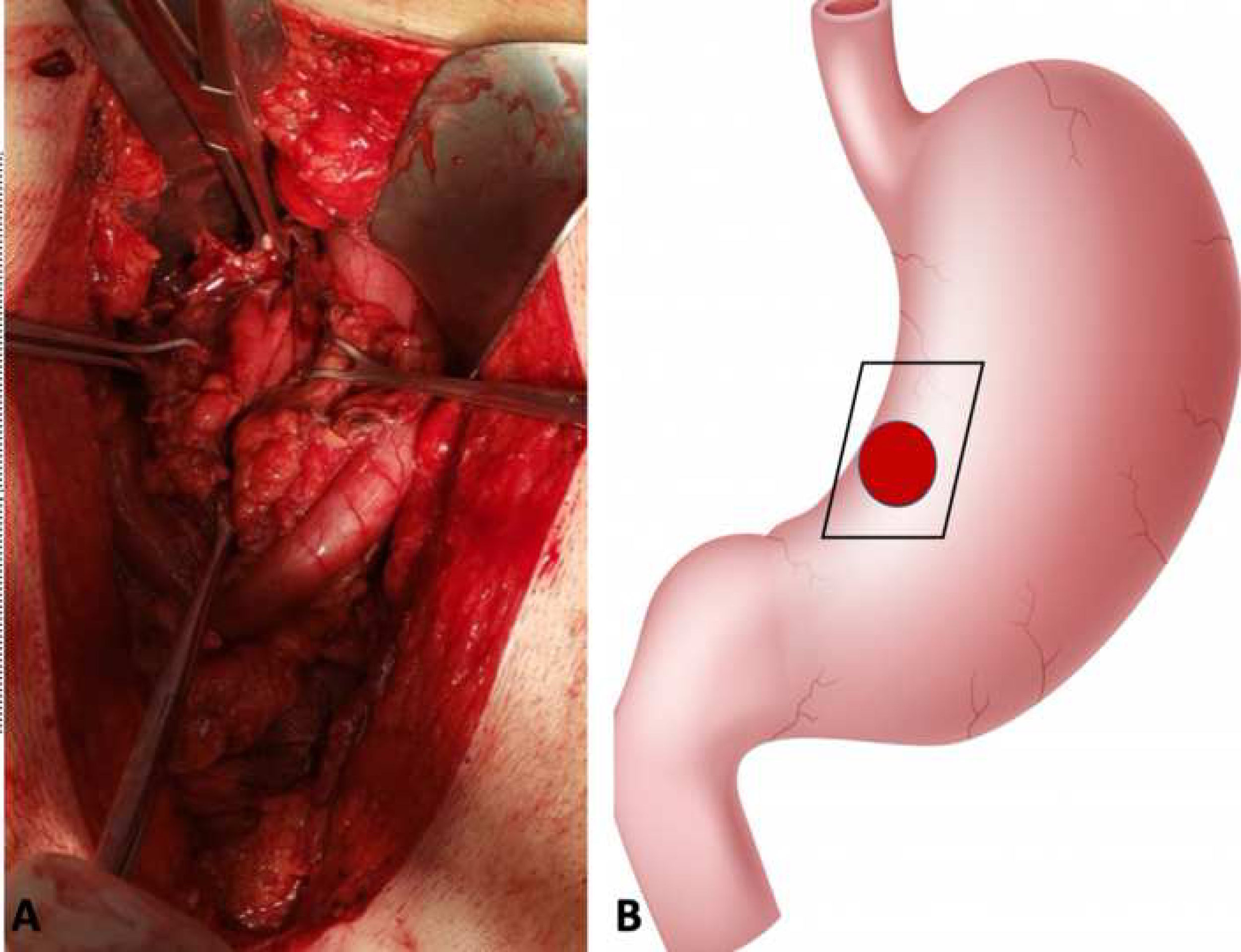
A 51-year-old man had illness onset 24 h prior to hospital admission. Upon ingesting sodium bicarbonate after having eaten an abundant amount of food, the patient had a sudden pain in the epigastrium, and went to the emergency department. He arrived conscious and aware of his surroundings, with a respiratory rate of 28 bpm, heart rate of 98 bpm, blood pressure of 130/98 mmHg, and temperature of 36.6 °C. His lungs were well ventilated, and his heart sounds had a regular rhythm. His abdomen was painful upon palpation and there were signs of peritoneal irritation in the four quadrants. Computed tomography showed intra-abdominal free air and identified gastric content leakage into the peritoneal cavity, as well as striation of the adjacent fat at the level of the lesser curvature (Fig. 1). The patient was taken to the operating room. A hollow organ perforation was revealed laparoscopically, showing free gastric fluid and generalized peritonitis. A perforation measuring approximately 5 × 5 cm was viewed in the lesser curvature of the stomach (Fig. 2). The procedure was converted and supraumbilical laparotomy was performed. The cavity was washed and partial gastrectomy, encompassing the lesser curvature, was carried out. The pylorus was preserved, utilizing a GIA linear stapler (Medtronic, USA), as was intestinal transit. The patient was released after seven days of hospitalization, tolerating oral diet, and with no complications. The pathology study reported no inflammatory process and ruled out neoplasia or peptic acid disease. At the postoperative follow-up at six months, the patient had no complications.
 Axial view, B) Oblique view.")
 Rupture of the stomach in the lesser curvature, measuring 5 × 5 cm. B) Illustration. The red circle is the perforation site. The black rhombus indicates the resection margins.")
There are two theories that explain the pathogenesis of spontaneous rupture of the stomach: the mechanical theory and the atonic theory.3,4 The atonic theory, proposed by Brinton in 1859, postulates that after prolonged periods of fasting, the stomach undergoes atony and muscular atrophy, associated with gastric wall weakness and delayed gastric emptying. That theory is related to patients with anorexia nervosa and bulimia, in whom sudden abundant food ingestion results in acute gastric dilation, causing an increase in intragastric pressure that exceeds the gastric venous pressure, with consequent wall ischemia.1,2 In 1861, Karl Freiherr von Rokitansky postulated the mechanical theory, or superior mesenteric artery syndrome, in which the vascular compression of the duodenum causes acute gastric dilation.4,5 Both theories are related to acute gastric dilation, causing tissue ischemia due to reduced venous flow. Venous blood flow has been reported to require an intragastric pressure between 19−20 cm H2O, or 3–4 L of fluid in the stomach.3–6
There are few reports in the literature on spontaneous rupture of the stomach due to sodium bicarbonate ingestion. One study confirmed that adding sodium bicarbonate to 2–3 L of diluted hydrochloric acid is sufficient for creating a rupture in the stomach, and also showed that the most important factors before adding the sodium bicarbonate were the volume of the solution, the quantity of reactants, the volume of air in the mixture, and the partial pressure of CO2, plus the importance of the presence of food, alcohol, or carbonic anhydrase.6 Those authors concluded that the ingestion of large quantities of sodium bicarbonate, with a distended stomach full of air, food, or liquid, could be an important factor for gastric rupture because it causes the release of hundreds of milliliters of gas, in less than three minutes.7 Rupture can occur when intragastric pressure reaches 120 mmHg or 4 L of fluids.2,4 Several cases have been reported, in which rupture of the stomach was due to abundant food intake, prior to taking sodium bicarbonate. In the majority of cases, rupture occurred in the lesser curvature, as in our patient, because that area of the stomach is shaped like a sphere, causing greater tension, and in turn, higher pressure.8
We conclude that acute gastric perforation after sodium bicarbonate ingestion is a rare entity with a high mortality rate, if not diagnosed opportunely, just like all perforations of the stomach. It is of the utmost importance to include the etiology described herein in the differential diagnosis of sudden epigastric pain, in patients with a history of eating large quantities of food and using sodium bicarbonate as a medication, even if there is no history of an eating disorder.
Ethical considerationsThe authors declare that no experiments were conducted on humans or animals for the present study, that they have followed the protocols of their work center on the publication of patient data, and that they have preserved patient anonymity at all times. Informed consent was obtained from the patient described in the article.
Financial disclosureNo specific grants were received from public sector agencies, the business sector, or non-profit organizations in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Patiño-Gallegos JA, González-Urquijo M, Padilla-Armendáriz D, Leyva-Alvizo A. Ruptura espontánea gástrica secundaria a ingesta de bicarbonato. Rev Gastroenterol Méx. 2021;86:315–317.

