
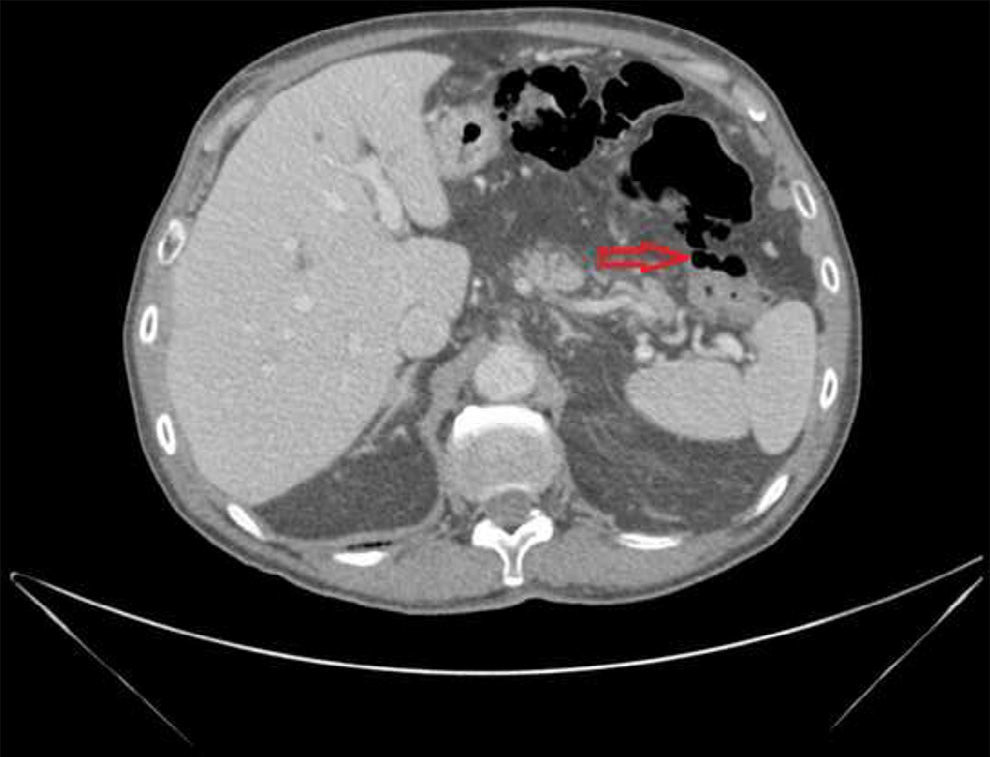
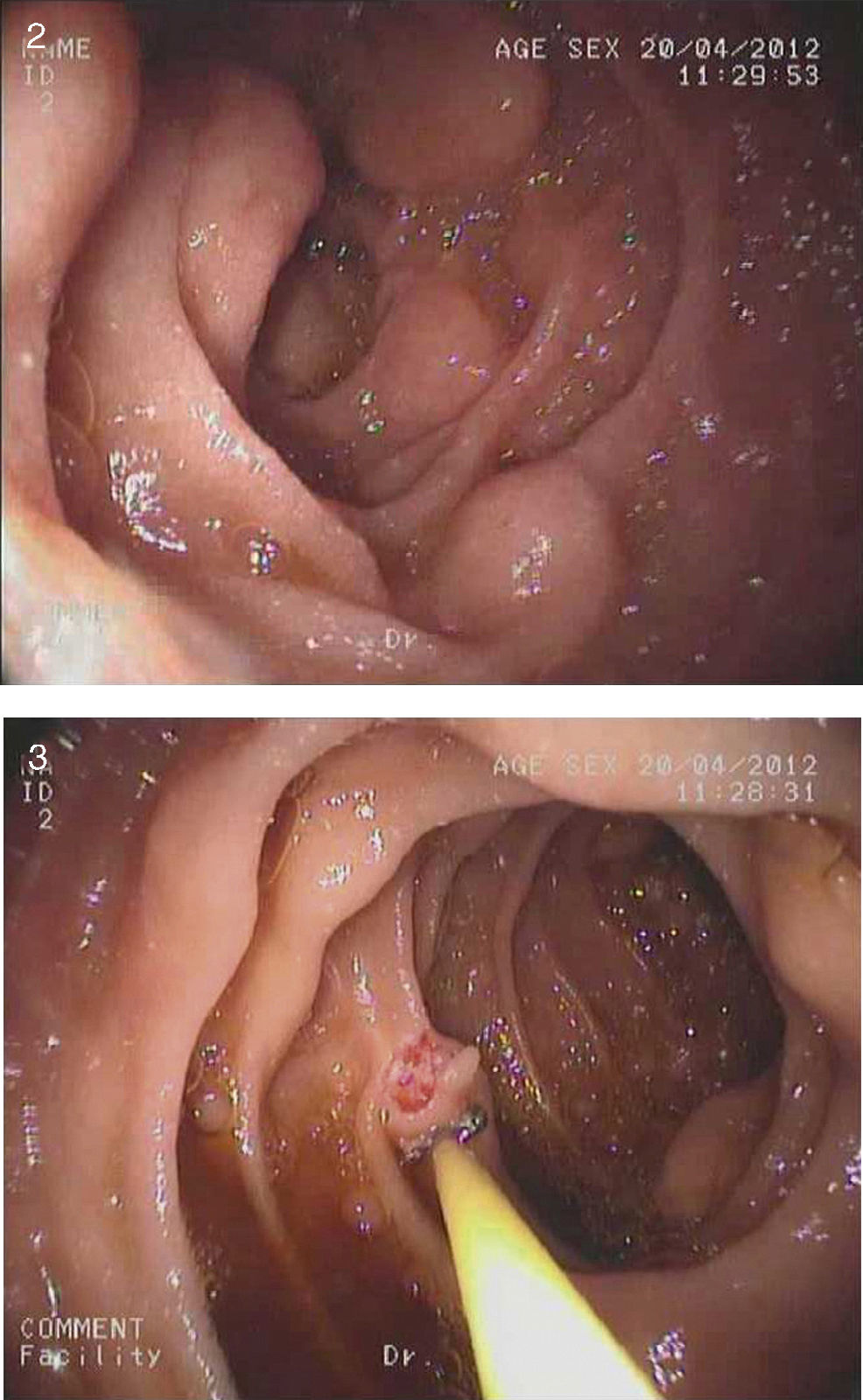
An 81-year-old man with an unremarkable medical history was in gastrointestinal follow-up consultation for constipation and recurrent abdominal pain. He arrived at the emergency department with intense non-radiating epigastric pain accompanied with nausea, but with no vomiting or fever. Physical examination revealed a distended and tympanic abdomen, reduced bowel sounds, generalized pain upon palpation, and no signs of peritoneal irritation. Blood analysis results reported increased acute phase reactants and pancreatic amylase (1.189 IU/l) and lipase (3.900 IU/l) in the acute pancreatitis range. After observing the pneumoperitoneum in a plain x-ray, an urgent abdominal CT scan was ordered that showed free intraperitoneal gas, mainly in the left flank, and thickening of the duodenum suggestive of peptic origin. There were no radiologic data of pancreatitis (fig. 1). Given the patient's clinical stability, he was admitted to the hospital with conservative management that consisted of digestive repose and wide-spectrum antibiotic therapy. At 48h the patient presented with important clinical improvement and with normal-range laboratory results. During his hospital stay, the etiologic study was completed and upper gastrointestinal endoscopy revealed numerous raised lesions in the bulb and second portion of the duodenum consistent with pneumatosis cystoides intestinalis (PCI) (figs. 2 and 3). These findings were confirmed through capsule endoscopy at the level of the jejunum. After completing the study, secondary causes were ruled out and the disease was classified as idiopathic. The patient presented with favorable progression with supplementary oxygen treatment and empirical antibiotic therapy and was asymptomatic upon his release from the hospital.


PCI is a rare entity characterized by the presence of multiple cysts in the wall of the gastrointestinal tract that are filled with air.1 Its precise etiology has not been clearly established nor is there a typical clinical presentation. Depending on its implicated cause, it can be described as primary or idiopathic (15%) and secondary (85%) in relation to abdominal diseases (surgical pathologies, infections, immunodeficiencies, or chronic inflammation) and extraintestinal pathologies.2 The diagnostic methods include radiologic studies, endoscopy, or surgery. Its significance and the need-to-treat must be evaluated in the clinical context. PCI does not often present with symptoms and if it does, they are usually nonspecific, such as abdominal discomfort, diarrhea, constipation, rectorrhagia, tenesmus, and weight loss; a small number of patients can present with severe complications such as tension pneumoperitoneum, hemorrhage, intussusception, or intestinal perforation. One of the pathognomonic signs observed in one third of the patients is the presence of pneumoperitoneum without peritoneal irritation due to a ruptured cyst.3
In our patient, the initial diagnosis was acute pancreatitis, given his clinical symptoms and the alterations in the laboratory test results, especially the increase in amylase and lipase. It was ruled out after we performed the imaging test that revealed the intra-abdominal free air that could justify the abovementioned alterations.
In regard to the therapeutic management of PCI, it should be directed at the underlying cause whenever possible. Asymptomatic patients do not require treatment and conservative management that includes steroids, basic diet, hyperbaric oxygen, and antibiotics is recommended in patients with mild symptoms. Surgical intervention is reserved for those cases that present with severe symptoms or complications.4
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Klimova K, Pérez Valderas MD, Merino Rodríguez B, González Asanza C, Menchén Fernández-Pacheco P. Neumatosis quística intestinal como causa infrecuente de dolor abdominal crónico. Revista de Gastroenterología de México. 2014;79:302–303.

