
Enteropathies are diseases that affect small bowel (SB) function and clinically manifest as chronic diarrhea and/or steatorrhea.1 They are a true clinical challenge, given their extensive differential diagnosis.
Monomorphic epitheliotropic intestinal T-cell lymphoma (MEITL) is a rare aggressive disease that mainly affects the SB mucosa. Its symptoms can be nonspecific, but often present as chronic diarrhea or steatorrhea. Diagnosis tends to be delayed, despite having distinctive histologic characteristics.
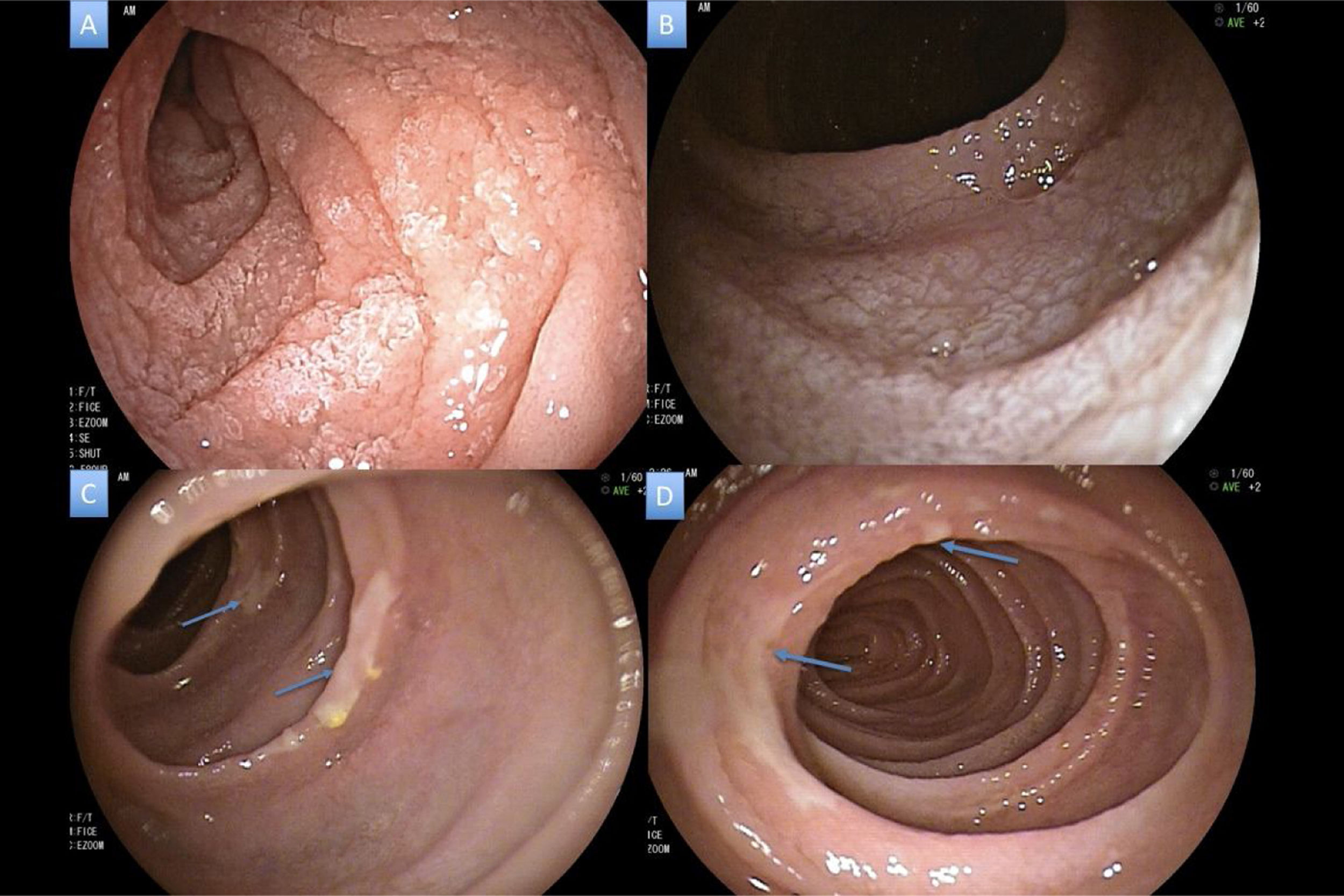
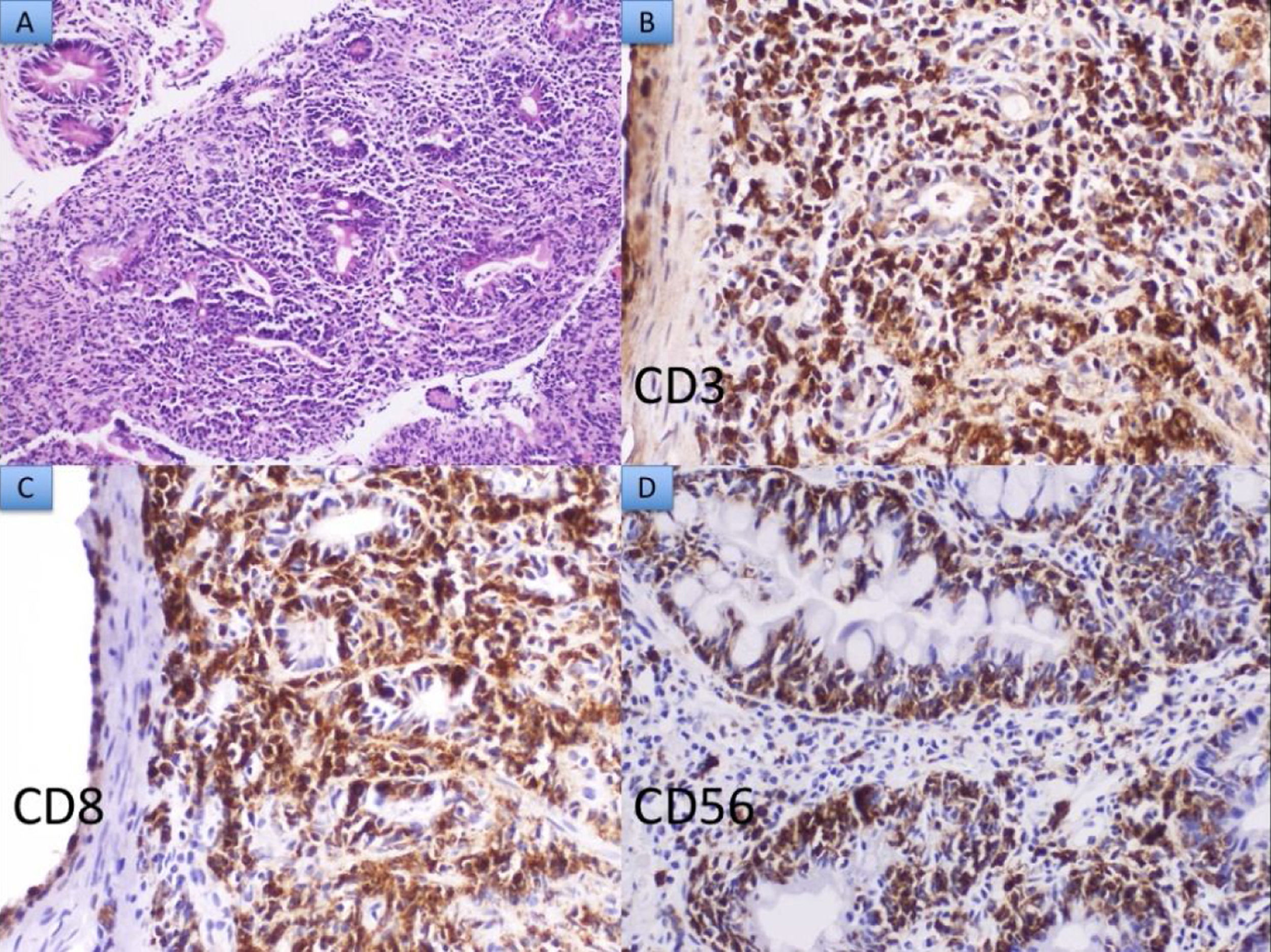
A 42-year-old man with alcohol use disorder presented with lienteric diarrhea and steatorrhea (on average 5–6 daily episodes), diffuse abdominal pain, edema, and weight loss of 20kg, over a 22-month period. Physical examination revealed a cachectic aspect, ascites, and edema of the extremities. Laboratory test results showed severe malnutrition due to hypoalbuminemia (1.8mg/dl) and anemia, with hemoglobin of 8.2g/dl. HIV ELISA test was negative. Initial endoscopic studies were normal, and biopsies were taken of the ileum and colon. The biopsy of the distal ileum revealed villous atrophy of the mucosa and infiltration of small lymphocytes in the lamina propria. Given those histologic findings, celiac disease was suspected, and the patient was started on a gluten-free diet, but his clinical condition remained the same. Deamidated gliadin peptide antibody and tissue transglutaminase antibody tests were negative. Anterograde enteroscopy identified inflammatory changes and villous atrophy in the distal duodenum and in the jejunum (Fig. 1A–D). Biopsies revealed a dense and monotonous infiltrate of small lymphocytes, with exocytosis into the epithelium and crypt destruction. Through immunohistochemistry, those lymphocytes expressed the CD3, CD7, CD8, and CD56 markers. They were negative for CD4 and perforin and the CD5 T-cell marker was lost. Ki-67 showed high proliferative activity. Those findings are characteristic of MEITL (Fig. 2A–D). No adenopathy or organomegaly was reported in the staging studies, but the bone marrow was infiltrated by atypical lymphocytes possessing the same intestinal immunophenotype.
 Segmental atrophy in the distal duodenum, B) Changes due to severe, homogeneous atrophy in the jejunum, C and D) Thinning of the mucosa in the mid jejunum with the presence of fibrin-covered superficial ulcerations in patches (blue arrows).")
 Hematoxylin and eosin ×20: Dense lymphoid infiltrate composed of medium-sized monomorphic lymphoid cells. B, C, and D) Neoplastic cells express the CD3, CD8, and CD56 markers, respectively.")
The patient’s progression during hospitalization was poor. He presented with Wernicke’s encephalopathy, gastrointestinal bleeding, and finally death, due to sepsis secondary to Staphylococcus aureus bacteremia, without having begun chemotherapy.
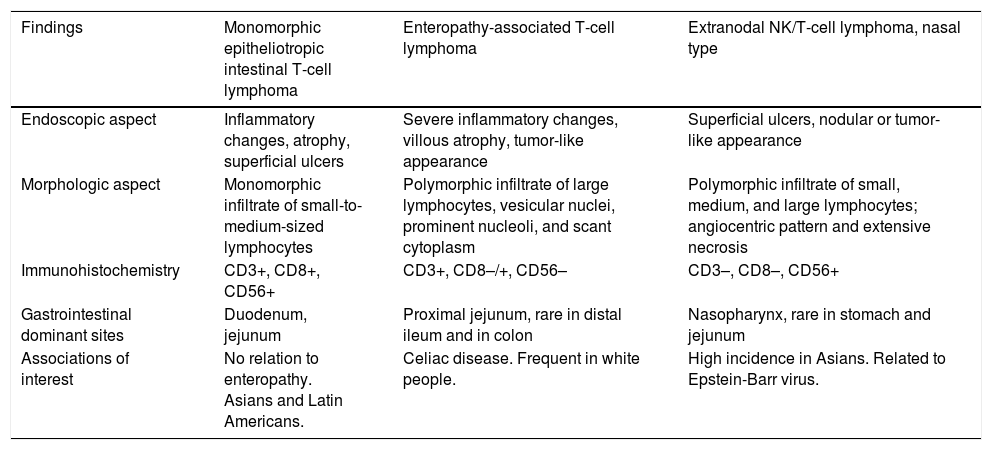
The differential diagnosis of enteropathy with steatorrhea is very broad and includes immune system-mediated causes, such as celiac disease, Crohn’s disease, and autoimmune enteropathy; drug-related causes; infiltrative causes, such as amyloidosis, eosinophilic enteritis, and collagenous sprue; infectious causes, such as HIV enteropathy, tropical sprue, giardiasis, Whipple disease, and tuberculosis; and rare causes, such as diffuse large B-cell lymphoma, enteropathy-associated T-cell lymphoma (EATL), and MEITL.1 The presence of intraepithelial lymphocytosis significantly reduces the differential diagnosis to celiac disease, drug-induced enteropathy, EATL, and MEITL. Those diseases should be distinguished by immunohistochemical markers. The most useful in the differential diagnosis of lymphoma-associated intraepithelial lymphocytosis are CD3, CD8, and CD56 (Table 1).
Differential diagnosis in intraepithelial lymphocytosis associated with lymphoma.
| Findings | Monomorphic epitheliotropic intestinal T-cell lymphoma | Enteropathy-associated T-cell lymphoma | Extranodal NK/T-cell lymphoma, nasal type |
|---|---|---|---|
| Endoscopic aspect | Inflammatory changes, atrophy, superficial ulcers | Severe inflammatory changes, villous atrophy, tumor-like appearance | Superficial ulcers, nodular or tumor-like appearance |
| Morphologic aspect | Monomorphic infiltrate of small-to-medium-sized lymphocytes | Polymorphic infiltrate of large lymphocytes, vesicular nuclei, prominent nucleoli, and scant cytoplasm | Polymorphic infiltrate of small, medium, and large lymphocytes; angiocentric pattern and extensive necrosis |
| Immunohistochemistry | CD3+, CD8+, CD56+ | CD3+, CD8–/+, CD56– | CD3–, CD8–, CD56+ |
| Gastrointestinal dominant sites | Duodenum, jejunum | Proximal jejunum, rare in distal ileum and in colon | Nasopharynx, rare in stomach and jejunum |
| Associations of interest | No relation to enteropathy. Asians and Latin Americans. | Celiac disease. Frequent in white people. | High incidence in Asians. Related to Epstein-Barr virus. |
NK: natural killer.
T-cell lymphomas account for just 5% of gastrointestinal tract lymphomas (EATL and MEITL). EATL corresponds to nearly 90% of cases, is associated with celiac disease, tends to present in Whites, and is histologically characterized by a polymorphous infiltrate with numerous eosinophils and plasmacytes that can hide neoplastic lymphoid cells. MEITL is an aggressive pathology with poor outcome and predominates in Asian and Latin American males. Its median survival rate is usually 7 months.2 At present, only one case has been reported in Colombia.3 The disease is not linked to celiac enteropathy, albeit a few cases have been described with said association.2 Interestingly, in Asia, where celiac disease is very rare, almost all cases of intestinal T-cell lymphoma are regarded as MEITL.4 Endoscopic findings of MEITL are inflammatory changes, such as edema, erythema, granularity, and superficial inflammatory ulcers.5 It spreads diffusely in the mucosa, with or without tumor-like lesions, unlike EATL, which is frequently associated with large tumors of the SB that tend to become perforated.2 MEITL used to be considered a type II EATL, but its distinctive immunophenotypic and morphologic findings have enabled the clear differentiation between the two pathologies. In addition, the genomic hybridization technique frequently shows an 8q24 gain in MEITL, resulting in the definition of a different genomic profile.6,7
There is no standard treatment for the disease. Multiple chemotherapy regimens have been utilized that are based on cyclophosphamide, doxorubicin, vincristine, and prednisolone (CHOP), PEG-asparaginase, pralatrexate, or autologous bone marrow transplantation, with varying efficacy.
In conclusion, MEITL is a rare entity, described in Asian and Latin American individuals, with a poor outcome and high mortality rate. Its clinical manifestations are diverse and its histopathologic findings distinctive, such as intraepithelial lymphocytosis with small-to-medium sized lymphocytes that are positive for CD3, CD8, and CD56. Those findings make the differential diagnosis of intraepithelial lymphocytosis a necessity in the clinical setting of chronic diarrhea and/or steatorrhea.
Ethical disclosuresThe present work meets the current bioethics research regulations and was authorized by the institutional ethics committee. A written statement of informed consent was not requested, given that the data are carefully protected. No data from the clinical history or imaging studies could identify the patient described in the clinical case.
The authors declare that the present article contains no data that could identify the patient.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Ramírez-Quintero JD, Carvajal JJ, Echeverri C, Mosquera-Klinger G. Linfoma T intestinal monomórfico epiteliotrópico en un paciente con diarrea crónica y esteatorrea. Revista de Gastroenterología de México. 2021;86:319–322.

