
There is no systematized information for determining/monitoring the burden of inflammatory bowel disease in Mexico. The aim of the present study was to estimate the annual burden of inflammatory bowel disease on the Mexican National Healthcare System, by number of patients seen, hospitalizations, and specific deaths, stratified into age groups.
Materials and methodsUtilizing specific databases of the Mexican National Healthcare System registries coded as ICD-10: K50 and K51, we retrieved and analyzed the data corresponding to the patients seen and hospitalized in 2015, stratified by age group, as well as the specific deaths. Treatment trends among physicians were also examined.
ResultsIn 2015, 5009 women (8.1) and 4944 men (8.4) with Crohn's disease received medical attention (prevalence of cases seen) and 35.1% of those patients were ≥50 years of age. In that same period, 17,177 women (27.7) and 15,883 men (26.9) with ulcerative colitis were seen and 31.6% of those patients were ≥50 years of age. The hospitalized cases (prevalence of hospitalized cases) were 1097 patients (0.91) with Crohn's disease and 43.7% of those patients were ≥50 years of age; and 5345 patients (4.42) with ulcerative colitis and 47.6% of those patients were ≥50 years of age. Deaths (specific mortality rate) were: 32 women (0.52) and 36 men (0.50) due to Crohn's disease, and 267 women (4.31) and 186 men (3.15) due to ulcerative colitis.
ConclusionsInflammatory bowel disease is a burden on the health of Mexican adults and the Mexican National Healthcare System, and it is expected to increase over the next 15 years.
En México no existe información sistematizada para determinar/monitorizar la carga de la enfermedad inflamatoria intestinal (EII). El objetivo del estudio fue estimar la carga anual de la EII en el Sistema Nacional de Salud por número de pacientes atendidos, hospitalizaciones y muertes y por grupos de edad.
Material y métodosUtilizando registros específicos de bases de datos del Sistema Nacional de Salud codificados por CIE-10: K50 y K51, obtuvimos y analizamos datos correspondientes a los pacientes atendidos y hospitalizados por grupo etario, así como muertes específicas durante el año 2015. Asimismo, se exploró la tendencia de tratamiento entre médicos.
ResultadosEn 2015, el número total de casos atendidos (prevalencia de casos atendidos) fue: enfermedad de Crohn en mujeres 5,009 (8.1), en hombres 4,944 (8.4). Los pacientes ≥50 años representaron el 35.1% del total; colitis ulcerosa crónica idiopática en mujeres 17,177 (27.7), en hombres 15,883 (26.9). Los ≥50 años representaron el 31.6% del total. Los casos hospitalizados fueron (prevalencia de casos hospitalizados): enfermedad de Crohn 1,097 (0.91). Los pacientes ≥50 años representaron el 43.7% del total; colitis ulcerosa crónica idiopática 5,345 (4.42). Los enfermos ≥50 años representaron el 47.6% del total. Las defunciones fueron (tasa de muertes específicas): en enfermedad de Crohn: mujeres 32 (0.52), hombres 36 (0.50); colitis ulcerosa crónica idiopática en mujeres 267 (4.31), en hombres 186 (3.15).
ConclusionesLa EII representa una carga para la salud de los adultos mexicanos y el Sistema de Salud, y se espera que aumente en los próximos 15 años.
Ulcerative colitis (UC) and Crohn's Disease (CD) are the two main forms of inflammatory bowel disease (IBD). Despite some common characteristics, they can be distinguished from one another by differences in genetic predisposition, risk factors, and clinical, endoscopic, and histologic findings. Although the exact cause of IBD is unknown, genetically susceptible individuals appear to have a dysregulated immune response in the mucosa and gut microbiota, resulting in bowel inflammation.1 Another distinctive feature of IBD is its epidemiologic profile, which varies geographically, imposing a serious burden upon the health systems of both developing and industrialized countries.
Since the beginning of the 21st century, IBD has become a worldwide public health problem,2,3 given the high number of cases, high hospitalization rates, disability, premature mortality, and an increase in direct medical cost with the advent of biologic therapy.4 In North America and Europe alone, around 1.5 million and 2 million people, respectively, suffer from the disease.3 Although the incidence of CD and UC is stabilizing in Western countries, the burden of disease remains on the rise because its prevalence continues to grow, consuming healthcare resources.2,3 At the same time, the incidence of IBD may be increasing rapidly in South America, Eastern Europe, Asia, and Africa,3 compared with Western societies. Indeed, the incidence of IBD is increasing in the developing world and in regions in the process of cultural westernization.3 Such is the case of Latin America, where countries like Brazil have experienced an annual growth in the incidence of IBD.5 For example, the incidence of CD increased by 42.2% in Spain, whereas it increased by 140.6% in Latin America. Similarly, the incidence of UC increased by 87.8% in Spain, compared with 333.3% in Latin America, highlighting contrasting trends in two populations of Hispanic origin.6 However, the lack of data in countries like Mexico, creates a challenge for understanding the burden of IBD in Latin America.
Previous studies on IBD in Mexico mirror the epidemiologic profile of the region but have methodological shortcomings. Yamamoto-Furusho7 found that the average annual number of new cases increased from 28.8 (1987–1996) to 76.1 (1997–2006), signifying a 2.6-fold increase in the average annual incidence, comparing both periods (p<0.00008). In addition, Bosques-Padilla et al.8 found that in 5 years (2004–2008), the adjusted annual rate of hospitalizations due to UC in the internal medicine service at a tertiary care hospital center in Northwest Mexico, was 2.3, 2.6, 3.0, 3.6, and 4.1/1000 hospitalizations, respectively, representing a 1.7-fold increase and raising the annual average of new cases from 17 to 29 (p<0.05). Unfortunately, those studies were conducted at single centers and so may not fully represent the epidemiology of the country. Moreover, the detailed epidemiologic information required to assess IBD on a greater scale could not be included in those studies due to their design.
Given the current increase in incidence, prevalence, mortality, and healthcare resources needed for the management of IBD worldwide, and the incremental behavior of those indicators, particularly in Latin America, along with the lack of updated national information in Mexico that can be systematized, monitored, and thus compared and managed, we decided to locally investigate different aspects of the disease.
Based on the abovementioned, our aim was to estimate the burden of disease of IBD in Mexico and examine the behavior of disease activity, as well as its specific treatment.
Materials and methodsFor the construction of the epidemiologic and patient care data (inpatients and outpatients), a retrospective analysis of local data sources from the national health system was conducted to estimate the burden of disease of IBD in Mexico. Data were stratified by age groups, to reveal the prevalence rates of patient care (inpatients and outpatients), as well as reported deaths from that cause, to recognize the 2015 annual burden of IBD in Mexico. In addition, to estimate the distribution of IBD patients by severity and clinical activity, as well as by type of treatment, physicians experienced in the treatment of patients with IBD were interviewed.
The data sources consulted were different health and information agencies within the Mexican healthcare system, obtaining the specific relevant information, either online or by special written request (institutional yearbooks and institutional statistics reports, statistical reports of morbidity and hospitalization from the national system of health information, health statistics from private institutions, cause-specific mortality statistics, etc.).9–14 The population pyramid of Mexico, specific and updated to 2015 (by sex and age groups), was obtained from official Mexican government sources.15,16
Because neither formal epidemiologic studies, nor population-based up-to-date registries in which the patient is followed clinically for a certain period, are available systematically for the diagnosis of IBD in Mexico, it was decided to estimate a surrogate prevalence of the pathologies (CD and UC) with a proxy variable. The information taken as the proxy variable was the total number of patients with CD (ICD-10: K50) or UC (ICD-10: K51) that received medical attention within the national healthcare system for a complete year (2015), based on the fact that it could be standardized, and thus compared with different healthcare systems (countries), as well as at different periods on the timeline. Thus, the prevalence of cases of CD and UC seen over a one-year period was estimated.
To obtain the total number of cases of CD and UC (ICD-10 code K50; K51) registered as having received medical attention for one year (inpatients and outpatients) within the Mexican health system, specific databases and queries of reported CD and UC cases were employed. We searched for the cases reported in 2015 by the ICD-10 codes: K50.0, K50.1, K50.8, and K50.9 for CD; and K51.0, K51.1, K15.7, K51.3, K51.4, K51.5, K51.8, and K57.9 for UC, by sex and age group. The data were collected by age group, as follows: <20, 20–29, 30–39, 40–49, 50–59, 60–69, and ≥70 years. The number of cases in each age group were then divided into the population of each age group/100,000 inhabitants, obtaining the prevalence rate of patients that received medical attention within the Mexican healthcare system for 100,000 person-years.
The total number of specific deaths registered (ICD-10: K50.0, K50.1, K50.8, and K50.9 for CD; and K51.0, K51.1, K15.7, K51.3, K51.4, K51.5, K51.8, and K57.9 for UC) was obtained from the corresponding official Mexican source.9 Said number (total deaths due to CD or UC as the primary cause, respectively) was divided into the population/100,000 inhabitants, for each age group, estimating both the total and the specific mortality rate by age group for Mexico (2015).
Given that IBD is not a disease that requires mandatory reporting in Mexico, it was not possible to gather information in that manner to estimate the incidence of ICD-10: K50; K51. In addition, the ICD-10: K50; K51 coded registries from the healthcare system databases of the patients seen do not distinguish between a new or subsequent patient, and so it was not possible to construct a rate of incidence of the condition.
Statistical analysisFor the distribution of patients by clinical status and type of treatment, a panel of specialists with extensive experience in IBD treatment was created. A specific instrument for data collection was designed, which was applied to the panelists according to the Delphi methodology.17 The questions were prepared on the basis of a focused review of the national and international medical literature available up to 2017.18–24 A basic statistical analysis was carried out on the resulting information, estimating central tendency measures (mean) and dispersion (standard deviation and 95% confidence intervals). The panel included physicians from the private and public sectors within the national health system. The sample size was not statistically representative, given that the purpose of the exercise was to obtain information of a qualitative nature to demonstrate a trend.
Finally, the total number of CD and UC patients that received medical attention (ICD-10 coded registries) in 2015 was obtained by age group and sex, and distributed by clinical status and type of treatment, according to the information from the Delphi panel.
Ethical considerationsThe sources of information of the present study were: administrative healthcare databases (public and open access), corresponding to Irreversibly Dissociated Anonymized Records (IDAR), which do not allow access to personal data that may be associated with an identifiable person; a bibliographic review; and a Delphi panel of physicians. Therefore, it was exempt from the need for review by an ethics committee.
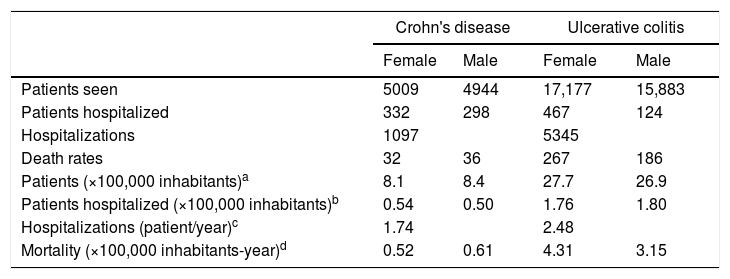
ResultsWithin the year 2015, 9953 cases with CD and 33,060 cases with UC (ICD-10: K50 and K51) received medical attention. Accordingly, the prevalence of cases seen (cases seen/100,000 inhabitants) was the following: CD, 8.1 for women and 8.4 for men; UC 27.7 for women and 26.9 for men (Table 1). There were 1097 hospitalized cases with CD and 5345 with UC in 2015, with a prevalence of hospitalization (hospitalized cases/100,000 inhabitants) of 0.54 for women and 0.50 for men with CD and 1.76 for women and 1.80 for men with UC. The average hospitalization rate per inpatient case (number of hospitalizations in one year/number of yearly inpatients) was 1.74 (CD) and 2.48 (UC) (Table 1). In the entire year, 68 deaths from CD were reported, with a rate of 0.52 for women and 0.61 for men (mortality by ICD-10: K50/100,000 persons-year). There were 453 deaths from UC, with rates of 4.31 and 3.15 for women and men, respectively (mortality by ICD-10: K51/100,000 persons-year). The information refers to primary causes of death in the register (Table 1).
Inflammatory bowel disease in Mexico in 2015: patients seen, patients hospitalized, and cause-specific deaths.
| Crohn's disease | Ulcerative colitis | |||
|---|---|---|---|---|
| Female | Male | Female | Male | |
| Patients seen | 5009 | 4944 | 17,177 | 15,883 |
| Patients hospitalized | 332 | 298 | 467 | 124 |
| Hospitalizations | 1097 | 5345 | ||
| Death rates | 32 | 36 | 267 | 186 |
| Patients (×100,000 inhabitants)a | 8.1 | 8.4 | 27.7 | 26.9 |
| Patients hospitalized (×100,000 inhabitants)b | 0.54 | 0.50 | 1.76 | 1.80 |
| Hospitalizations (patient/year)c | 1.74 | 2.48 | ||
| Mortality (×100,000 inhabitants-year)d | 0.52 | 0.61 | 4.31 | 3.15 |
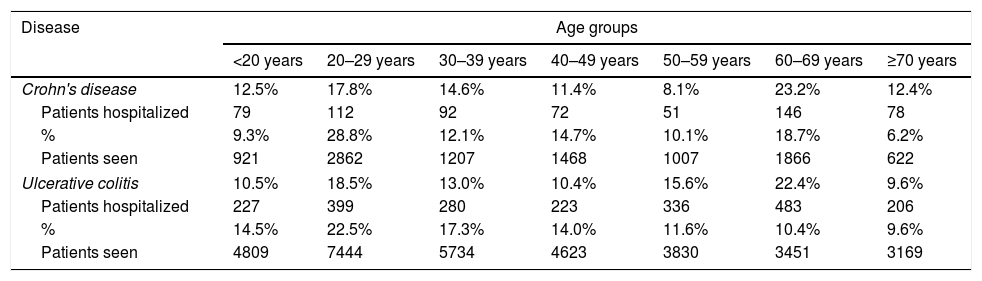
By age group, it was apparent both in UC and CD that the peak was in the group of 20–40 years of age (39.9 and 40.9%, respectively). For hospitalized patients, the curves showed two concentration peaks: in CD in the groups ≥60 years of age (35.6%) and 20–40 years of age (32.4%), and in UC in the groups ≥60 years of age (32.0%) and 20–40 years of age (31.5%) (Table 2).
Inflammatory bowel disease in Mexico in 2015: patients seen and hospitalized, by age group.
| Disease | Age groups | ||||||
|---|---|---|---|---|---|---|---|
| <20 years | 20–29 years | 30–39 years | 40–49 years | 50–59 years | 60–69 years | ≥70 years | |
| Crohn's disease | 12.5% | 17.8% | 14.6% | 11.4% | 8.1% | 23.2% | 12.4% |
| Patients hospitalized | 79 | 112 | 92 | 72 | 51 | 146 | 78 |
| % | 9.3% | 28.8% | 12.1% | 14.7% | 10.1% | 18.7% | 6.2% |
| Patients seen | 921 | 2862 | 1207 | 1468 | 1007 | 1866 | 622 |
| Ulcerative colitis | 10.5% | 18.5% | 13.0% | 10.4% | 15.6% | 22.4% | 9.6% |
| Patients hospitalized | 227 | 399 | 280 | 223 | 336 | 483 | 206 |
| % | 14.5% | 22.5% | 17.3% | 14.0% | 11.6% | 10.4% | 9.6% |
| Patients seen | 4809 | 7444 | 5734 | 4623 | 3830 | 3451 | 3169 |
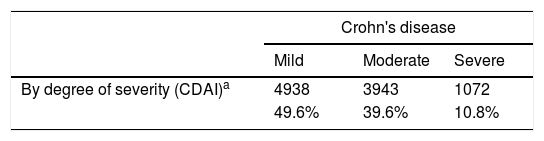
The distribution of patients by severity or activity in accordance with the most widely used measurement scales18–24 was: in the cases with CD, 50.4% of the patients were classified as moderate-to-severe (Crohn's disease activity index [CDAI]), and 66.2% as moderately active-markedly active (Harvey Bradshaw index [HBI]). In the cases with UC, 48.0% of the patients were ranked as moderate-to-severe (Truelove and Witts criteria), and 69.3% in grades 2–3 of the Mayo scale (Table 3).
Inflammatory bowel disease in Mexico in 2015: patients by disease severity or activity.
| Crohn's disease | |||
|---|---|---|---|
| Mild | Moderate | Severe | |
| By degree of severity (CDAI)a | 4938 | 3943 | 1072 |
| 49.6% | 39.6% | 10.8% | |
| % | Remission | Moderately active | Markedly active |
|---|---|---|---|
| By simplified index of activity (HBI)b | 3369 | 6345 | 239 |
The site of patient care and hospitalization had the following distribution: for CD, of the 9953 cases seen, 2128 (21.4%) corresponded to the private sector and 7825 (78.6%) to the public sector, and of the 630 hospitalized cases, 117 (18.6%) were from the private sector, and 513 (81.4%) from the public sector; for UC, of the 33,060 cases seen, 6142 (18.6%) were from the private sector and 29,918 (81.4%) from the public sector, and of the 2154 hospitalized cases, 450 (20.9%) were from the private sector, and 1704 (79.1%) from the public sector.9–14
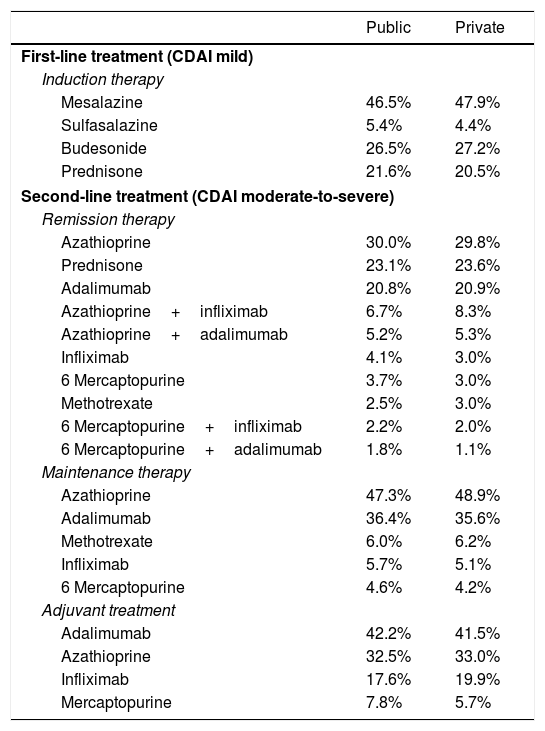
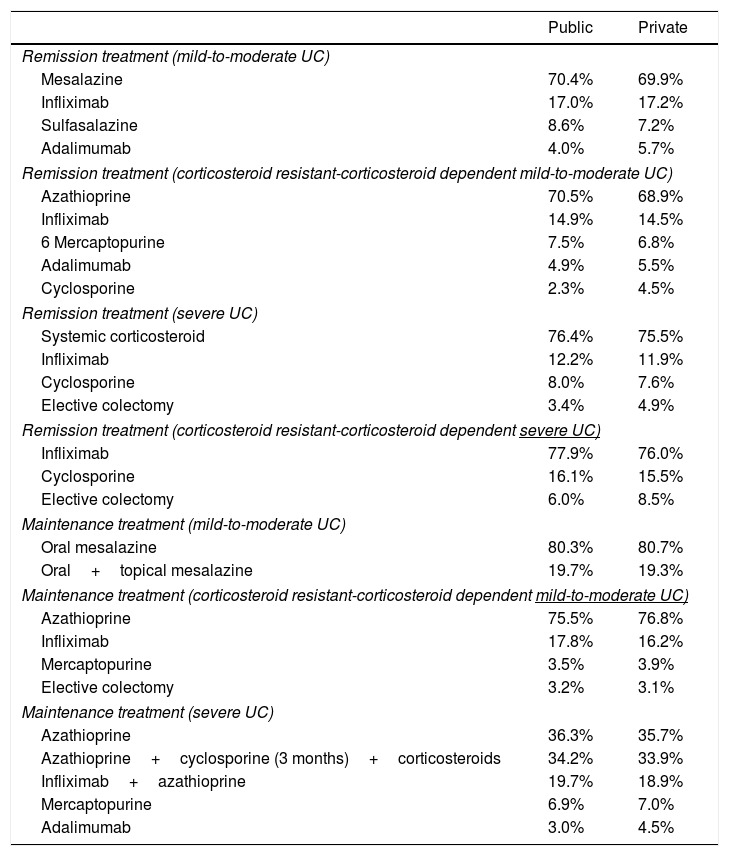
In Tables 4 and 5, the distribution of the different treatments is presented according to disease severity and activity, and to the healthcare setting. Anti-TNF therapy was used in an average of 28% of the cases of CD (in both the public and private sectors), whereas it was used in 19% of the cases of UC (in both the public and private sectors).
Inflammatory bowel disease in Mexico in 2015: Crohn's disease, treatment by clinical status, and healthcare setting.
| Public | Private | |
|---|---|---|
| First-line treatment (CDAI mild) | ||
| Induction therapy | ||
| Mesalazine | 46.5% | 47.9% |
| Sulfasalazine | 5.4% | 4.4% |
| Budesonide | 26.5% | 27.2% |
| Prednisone | 21.6% | 20.5% |
| Second-line treatment (CDAI moderate-to-severe) | ||
| Remission therapy | ||
| Azathioprine | 30.0% | 29.8% |
| Prednisone | 23.1% | 23.6% |
| Adalimumab | 20.8% | 20.9% |
| Azathioprine+infliximab | 6.7% | 8.3% |
| Azathioprine+adalimumab | 5.2% | 5.3% |
| Infliximab | 4.1% | 3.0% |
| 6 Mercaptopurine | 3.7% | 3.0% |
| Methotrexate | 2.5% | 3.0% |
| 6 Mercaptopurine+infliximab | 2.2% | 2.0% |
| 6 Mercaptopurine+adalimumab | 1.8% | 1.1% |
| Maintenance therapy | ||
| Azathioprine | 47.3% | 48.9% |
| Adalimumab | 36.4% | 35.6% |
| Methotrexate | 6.0% | 6.2% |
| Infliximab | 5.7% | 5.1% |
| 6 Mercaptopurine | 4.6% | 4.2% |
| Adjuvant treatment | ||
| Adalimumab | 42.2% | 41.5% |
| Azathioprine | 32.5% | 33.0% |
| Infliximab | 17.6% | 19.9% |
| Mercaptopurine | 7.8% | 5.7% |
Inflammatory bowel disease in Mexico in 2015: ulcerative colitis (UC), treatment by clinical status, and healthcare setting.
| Public | Private | |
|---|---|---|
| Remission treatment (mild-to-moderate UC) | ||
| Mesalazine | 70.4% | 69.9% |
| Infliximab | 17.0% | 17.2% |
| Sulfasalazine | 8.6% | 7.2% |
| Adalimumab | 4.0% | 5.7% |
| Remission treatment (corticosteroid resistant-corticosteroid dependent mild-to-moderate UC) | ||
| Azathioprine | 70.5% | 68.9% |
| Infliximab | 14.9% | 14.5% |
| 6 Mercaptopurine | 7.5% | 6.8% |
| Adalimumab | 4.9% | 5.5% |
| Cyclosporine | 2.3% | 4.5% |
| Remission treatment (severe UC) | ||
| Systemic corticosteroid | 76.4% | 75.5% |
| Infliximab | 12.2% | 11.9% |
| Cyclosporine | 8.0% | 7.6% |
| Elective colectomy | 3.4% | 4.9% |
| Remission treatment (corticosteroid resistant-corticosteroid dependent severe UC) | ||
| Infliximab | 77.9% | 76.0% |
| Cyclosporine | 16.1% | 15.5% |
| Elective colectomy | 6.0% | 8.5% |
| Maintenance treatment (mild-to-moderate UC) | ||
| Oral mesalazine | 80.3% | 80.7% |
| Oral+topical mesalazine | 19.7% | 19.3% |
| Maintenance treatment (corticosteroid resistant-corticosteroid dependent mild-to-moderate UC) | ||
| Azathioprine | 75.5% | 76.8% |
| Infliximab | 17.8% | 16.2% |
| Mercaptopurine | 3.5% | 3.9% |
| Elective colectomy | 3.2% | 3.1% |
| Maintenance treatment (severe UC) | ||
| Azathioprine | 36.3% | 35.7% |
| Azathioprine+cyclosporine (3 months)+corticosteroids | 34.2% | 33.9% |
| Infliximab+azathioprine | 19.7% | 18.9% |
| Mercaptopurine | 6.9% | 7.0% |
| Adalimumab | 3.0% | 4.5% |
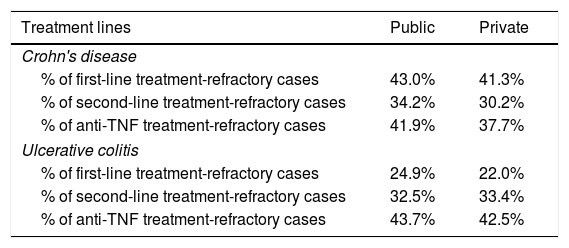
Table 6 shows the rates of treatment-refractory patients in relation to the different lines of treatment by healthcare setting.
Inflammatory bowel disease in Mexico in 2015: average rate of treatment-refractory cases.
| Treatment lines | Public | Private |
|---|---|---|
| Crohn's disease | ||
| % of first-line treatment-refractory cases | 43.0% | 41.3% |
| % of second-line treatment-refractory cases | 34.2% | 30.2% |
| % of anti-TNF treatment-refractory cases | 41.9% | 37.7% |
| Ulcerative colitis | ||
| % of first-line treatment-refractory cases | 24.9% | 22.0% |
| % of second-line treatment-refractory cases | 32.5% | 33.4% |
| % of anti-TNF treatment-refractory cases | 43.7% | 42.5% |
The present study investigated and analyzed indicators that enable assessment of the burden of IBD in Mexico, using the local information available. The study confirms the great variability of prevalence rates reported for IBD (for every 100,000 inhabitants), laying the groundwork for its economic evaluation in Mexico, as well as highlighting the increasing mortality rates due to IBD in Mexico. The average use of biologic therapy was higher in Mexico, compared with other populations. We discuss our findings with respect to previous evidence.
The results document a prevalence of CD ranging from 8.1 to 8.4, and UC from 26.9 to 27.7. Those data place Mexico within the range of Latin America and the regions in the process of westernization in general, although with marked differences. From a systematic review (1990–2016), Ng et al.3 recently reported (2017) a regional prevalence (for every 100,000 inhabitants) for IBD: in North America, a range of 96.3–318.5 for CD and 139.8–286.3 for UC; in Eastern Europe, 1.51–200.0 for CD and 2.42–340.0 for UC; in Africa, 19.02 for CD and 10.57 for UC; in South Asia, 1.2 for CD and 5.3–44.3 for UC; in Latin America, 0.9–41.4 for CD and 4.7–44.3 for UC.
Our findings described a bimodal distribution of hospitalizations for CD in young adults and the elderly. Hospitalizations due to UC also exhibited a curve with two peaks, similar to our findings on CD, but different from those of Sonnenberg. Regarding hospitalization distribution by age group, Sonnenberg25 analyzed 17 years of hospital discharges in England and Scotland and found a double peak pattern in CD (25–29 years, and 75–79 years) and one basically unimodal in UC, with the peak in older patients (≥75 years). Nevertheless, close to 50% of hospitalizations occurred in patients >50 years of age, and in CD the two peaks were situated in the age groups of 20–39 years and >60 years, respectively.
An experience in Chile was recently reported, with respect to hospitalizations for IBD, using the same methodology as in our study. Those authors compared the admission characteristics in patients hospitalized for IBD (ICD-10-CM K50 and K51) between two non-consecutive periods of 2 years each, selected at random: 2008 and 2009 versus 2013 and 2014. In the first period, the rate of hospitalizations due to IBD was 1.47/100,000 person-years. In the second, it was 3.25/100,000 person-years. That finding represents a 2.2-fold increase in the hospitalization rate (p<0.01) and the working-age population was the most affected.26 In our study, the rate of hospitalization for IBD corresponded to 1.55/100,000 person-years, but the trend shown in the Chilean study is similar to that reported by Bosques-Padilla.8
A systematic review was conducted on that same topic to identify population-based studies reporting hospitalization rates (or crude hospitalizations) after the year 2000, with at least 5 years of data. Log-linear models were used to calculate the average annual percentage change (AAPC), with associated 95% confidence intervals (CIs). Hospitalizations for IBD in North America and Europe were divergent, that is, they increased in some countries and decreased in others. In contrast, the results showed that although newly industrialized countries outside the Western world have the lowest hospitalization rates, those rates are rapidly increasing in South America (e.g., Mexico [2000–2015] AACP: 3.67; 95% CI: 2.8, 4.55), the Middle East (Bahrain), and Asia (China). Those rapidly rising hospitalization rates are contributing to an increasing burden on local healthcare systems.27
In 2015, we documented mortality rates of 0.56 and 3.7 for CD and UC, respectively. They represent a 2.44-fold increase in the mortality rate of CD over 10–25 years, and a 6.24-fold increase in the mortality rate of UC during the same period. We estimated the standardized mortality rate indirect (SMRI) for 2015, resulting in 1.26 for CD and 2.53 for UC, both in the total population. Regarding CD, incremental risk was situated mainly in the age group <60 years (particularly the group of 30–39 years of age [22.77]), whereas for UC, the incremental risk was distributed similarly in virtually all age groups. With respect to IBD mortality in Mexico, our research data showed a significant increase, when compared with the information reported by Sonnenberg.28 According to that source, in the period of 1991–2004 in Mexico, the mortality rate for CD was 0.23 (annual deaths per million living inhabitants) and for UC was 0.60. For that same indicator, Burisch et al. reported an SMRI for CD of 1.39 (95% CI, 1.30–1.49), and of 1.1 for UC (95% CI, 0.9 - 1.2) in the European Union (EU, pooled data 2013).29 That mortality data supports the increase in the burden of disease in Mexico.
Our findings are similar to those in the EU regarding CD, but are discordant with respect to UC, in which the burden due to increased risk vs. that of the general population is comparatively very high in Mexico. According to Sonnenberg,28 Mexico is in a range similar to that reported for CD in Hong Kong (0.58), Taiwan (0.45), and Japan (0.37) in the period of 1991–2004. In terms of UC, it positions Mexico at the level of Argentina (0.67) over the same period, as well.
With respect to the trend of treatment, the present study revealed a prescription of anti-TNF therapy in CD similar to or slightly higher than that reported in previous literature up to 2015. Van der Valk et al.30 reported the following use of anti-TNF therapy in Denmark (2011) in 1315 patients with CD: infliximab use in 10.4% and adalimumab in 12.3%, compared with the 22.7% and 28.2% in our study. In 937 patients with UC they found infliximab use in 3% and adalimumab in 1% (4%), whereas average use in our study was much higher at 19%.
Concerning the resistance to or failure of anti-TNF therapy, our results showed rates of 37.7% and 41.9% for CD and 42.5% and 43.7% for UC (private and public sectors, respectively), in line with the international literature consulted (36–40%).20
The total direct medical costs of IBD (2013) have been reported at around €1871 (SD €4884), with the cost of CD (€2548 per patient-year) higher than that of UC (€1574). In the pre-biologic era, hospitalization due to CD accounted for 63% of the total direct costs, whereas for UC it was 45%. With the use of anti-TNF therapy, medical treatment now represents 64% of the total direct medical cost of CD, and 31% of UC, with a per capita quarterly cost of €1626 for CD and €595 for UC.30 Thus, it is important to emphasize that IBD can be associated with significant financial costs, due to both the hospitalization rate and the specific treatment involving the use of biologic products. In addition, premature death and disability are associated with the loss of productivity.30 We did not analyze healthcare costs in our research.
Basically, the methodology utilized in our study was the use of the ICD-10 coded registries from the healthcare system sources (specific databases) and it should be mentioned that the administrative databases of the healthcare registries (outpatient cases, hospital cases, hospital discharges, diagnostic tests, procedures, etc.) have been in use for several years, in the Americas and in Europe.31 Among the different administrative health databases, hospital discharges have been the most widely used.31 Registries strengthen, validate, or even attempt to replace the population-based epidemiologic records, with applications including monitoring and surveillance.31,32 As a very recent example of those applications in Latin America, specifically in IBD, an analysis of hospitalizations was published from registers using ICD-10 codes in Chile.26 In addition, another recent report used the same methodology as our own to analyze the hospitalization for pneumonia among the elderly as information of morbidity and increased healthcare utilization.33
Administrative healthcare databases have strengths that enable them to serve multiple purposes, such as those mentioned above. They are also relatively inexpensive and easy to obtain and use, when compared with the cost and time invested to obtain the same data through other means, such as surveys or clinical record abstraction. Furthermore, they are considered more reliable than other data sources, such as self-reported patient outcomes, or physician round tables, that in general represent their specific experience with regard to disease surveillance and resource use. Administrative healthcare databases are generally available for several years, making trend analysis possible,32 and given their coverage of large populations, they can be used for the analysis of specific facts or population subgroups.
The thoroughness of employing administrative databases using ICD-coded registries as a method vs. a clinical one is accepted in several international studies, with a 70–90% correlation.33 In other words, with the method used in the present study, around 85% of the data is accepted by the international community, on average, as fully reliable. It has also been specifically stated that 80–90% of records coded as ICD-10 are correct in terms of their correlation with accepted clinical and paraclinical support.34 In addition, a 10–20% overestimation of IBD in highly industrialized countries has been found, a fact not seen in developing countries.34
Despite the considerable advantages of administrative healthcare databases, there are also weaknesses that may limit their usefulness for certain applications, such as differences in the methods and policies of collecting information among health systems and countries, consequently compromising database comparability. Said differences can lead to varying degrees of underreporting, albeit that phenomenon is internationally accepted to be limited to between 10 and 20%.
Those weaknesses are importantly minimized by using standardized and universally accepted classifications, such as the current ICD-10 coding, and through initiatives in some parts of the world to increase and improve the quality of the data available in the database registries.31
Finally, it is very clear (and totally coincident with the intention of the authors of the present manuscript) that IBD, in its different clinical-nosologic manifestations, must be registered directly, diligently, and systematically, in accordance with its presumed high individual and social costs related to health and quality of life, health resource use, and the impact on health systems, consequently reflecting its burden of disease for Mexican society in general. Simply stated, specific actions must be taken to increase the quality of the IBD records and registration processes.
In many cases, including the present study, the clinical and therapeutic information is not sufficiently detailed or robust, forcing the use of other alternative methods for obtaining said information. That information in our study was derived from a Delphi panel of physicians and must be considered qualitative, rather than quantitative data. The examination of clinical information and its correlation with the types of treatment presented herein is only an overview of the experience of a group of Mexican physicians in the public and private sectors. As an additional and complementary phase of the present study, deeper and more extensive research regarding therapy and its correlation with the clinical status of the patients should be developed, as well as an exercise in the cost component, to complete the analysis of the burden of IBD.
It is important to consider that our data refers to the prevalence of medical attention. That is to say, it only considers cases captured in the health system through registries from 2015.
According to the data obtained in our research and the results shown by other authors of studies carried out on different types of populations and geographic areas, it is clear that IBD shows an increasing trend worldwide, with Latin America as one of the regions with an accelerated expansion of cases, both at the present time and in the future.23 Together with the recognition of the epidemiologic trend of IBD in the Mexican environment, awareness of healthcare resource use (medical attention, hospitalization, etc.) related to patient age and sex, and knowledge of the specific mortality, are extremely important for estimating the burden of disease, in addition to having a better understanding of the problem. Ideally, in our environment, we must strive to know the different components from which we can build complex indicators that assess the burden of disease in an integral manner, such as the disability-adjusted life years (DALYs) (years of healthy life lost).
In our specific case, we consider that the analysis of the cases that received medical attention and the cases hospitalized, identified through ICD-10 coding (ICD-10: K50 and K51), can function as a proxy variable of disease prevalence, allowing different healthcare resource use metrics to be employed. Most importantly, it can facilitate the analysis of trends in the behavior of the condition, aiding in decision-making regarding the approach to IBD management, in the Mexican context.
We can conclude that several IBD metrics are changing, demonstrating its growth trend throughout the world, particularly in developing countries, with an emphasis on an upward trend in Latin America, including Mexico. Said conclusion can be drawn, despite having limited information and generally indirect measurements of the behavior of the cases, with discontinuity in the timeline. Those insufficiencies underline the need for more detailed knowledge of the phenomenon, going beyond the limited approach to determining indicators of incidence and prevalence, by covering information on specific mortality and health resource use and related costs, so that the burden of disease can be fully determined and better understood. That would enable long-term monitoring of IBD, resulting in better local management of the disease, as well as in systematic comparisons with the rest of Latin America and the world, in general.
Therefore, far from being discouraged by the lack of various elements of analysis, we are using those available to develop a methodology to assess, evaluate, and monitor the disease in the future, but starting now, with the possibility of international comparisons and discussions, and clearly with the aim of continuously improving the measurements.
At present, the authors maintain that the method utilized, and the information reported herein, are valuable and worthy of consideration, given the almost complete absence of systematized and comparable information on this topic in Mexico.
Author contributionsDr. Yamamoto-Furusho: study design and conceptualization, data interpretation, manuscript drafting, extensive participation in the critical review of the manuscript and the process of submission to the selected journal. He also approved the final draft.
Dr. Francisco Bosques: study conceptualization, data interpretation, manuscript drafting, extensive participation in the critical review of the manuscript. He approved the final draft.
Dr. Luis Charúa: study conceptualization, data interpretation, manuscript drafting, extensive participation in the critical review of the manuscript. He also approved the final draft.
Dr. Tomás Cortés: study conceptualization, manuscript drafting, extensive participation in the critical review of the manuscript. He also approved the final draft.
Dr. Rosa Maria Miranda: study conceptualization, manuscript drafting, extensive participation in the critical review of the manuscript. She also approved the final draft.
Dr. Yusimit Ledesma: study design and conceptualization, manuscript drafting, extensive participation in the critical review of the manuscript. She also approved the final draft.
Dr. Adolfo Saez: manuscript drafting and extensive participation in the critical review of the manuscript. He also approved the final draft.
FundingThe present study was carried out under the financing of Takeda México SA de CV, with no type of legal responsibility and/or responsibility related to the results.
Conflict of interestProfessor Jesús K. Yamamoto-Furusho has received honoraria from Abbvie, Takeda, Janssen, UCB, Alfa Sigma, Ferring, Almirall, Pfizer, Schwabe Pharma, Novartis, and Danone as a speaker, key opinion leader, and member of the advisory board at national and international levels. He has received research grants from Bristol, Shire, Pfizer, and Takeda. He is President of the Pan American Crohn's and Colitis Organisation (PANCCO).
Dr. Francisco J Bosques-Padilla has been a consultant for Takeda and Alfa Wassermann. He has also been a speaker for Takeda, Abbvie, MSD, and Janssen Cilag.
Dr. Luis Charúa-Guindic declares that he has no conflict of interest.
Dr. Tomas Cortés-Espinosa has been a speaker for Janssen Cilag and UCB.
Dr. Rosa Maria Miranda-Cordero has been a speaker for Abbvie, Janssen, and Ferring. She has served on the Janssen Regional Ulcerative Colitis advisory committee, in Washington DC, on May 17, 2015, on the Inflammatory Bowel Disease: Crohn's Disease advisory committee, in Amsterdam, Holland, on March 18, 2016, and on the Ustekinumab 2017 advisory committee, in Mexico City, on June 10, 2017.
Dr. Adolfo Saez was an employee of Takeda Mexico SA de CV, during the time of the study.
Dr. Yusimit Ledesma-Osorio was an employee of Takeda Mexico SA de CV, during the time of the study.
The authors wish to thank Links & Links for their support in carrying out this research, as well as for their assistance in drafting the present document.
Please cite this article as: Yamamoto-Furusho JK, Bosques-Padilla FJ, Charúa-Guindic L, Cortés-Espinosa T, Miranda-Cordero RM, Saez A, et al. Epidemiología, carga de la enfermedad y tendencias de tratamiento de la enfermedad inflamatoria intestinal en México. Revista de Gastroenterología de México. 2020;85:246–256.

