
Atrophy and intestinal metaplasia are early phenotypic markers in gastric carcinogenesis. White light endoscopy does not allow direct biopsy of intestinal metaplasia due to a lack of contrast of the mucosa. Narrow-band imaging is known to enhance the visibility of intestinal metaplasia, to reduce sampling error, and to increase the diagnostic yield of endoscopy for intestinal metaplasia in Asian patients. The aim of our study was to validate the diagnostic performance of narrow-band imaging using 1.5× electronic zoom endoscopy (with no high magnification) to diagnose intestinal metaplasia in Mexican patients.
Materials and methodsA retrospective cohort study was conducted on consecutive patients with dyspeptic symptoms at a private endoscopy center within the time frame of January 2015 to December 2016.
ResultsA total of 338 patients (63±8.4 years of age, 40% women) were enrolled. The prevalence of H. pylori infection was 10.9% and the incidence of intestinal metaplasia in the gastric antrum and corpus was 23.9 and 5.9%, respectively. Among the patients with intestinal metaplasia, 65.3% had the incomplete type, 42.7% had multifocal disease, and one third had extension to the gastric corpus. Two patients had low-grade dysplasia. The sensitivity of white light endoscopy was 71.2%, with a false negative rate of 9.9%. The sensitivity, specificity, positive predictive value, negative predictive value, and accuracy of narrow-band imaging (with a positive light blue crest) were 85, 98, 86.8, 97.7, and 87.2%, respectively.
ConclusionThe prevalence of H. pylori infection and intestinal metaplasia in dyspeptic Mexican patients was not high. Through the assessment of the microsurface structure and light blue crest sign, non-optical zoom narrow-band imaging had high predictive values for detecting intestinal metaplasia in patients from a general Western setting.
La atrofia y metaplasia intestinal son marcadores fenotípicos tempranos en la carcinogénesis gástrica. La endoscopia con luz blanca no permite la biopsia directa de metaplasia intestinal debido a la falta de contraste de la mucosa. Se sabe que la imagen de banda estrecha aumenta la visibilidad de metaplasia intestinal, reduce el error de muestreo e incrementa el rendimiento diagnóstico endoscópico para metaplasia intestinal en pacientes asiáticos. El objetivo de nuestro estudio fue validar la utilidad de la endoscopia con imagen de banda estrecha para el diagnóstico de metaplasia intestinal en pacientes mexicanos utilizando un endoscopio con zoom electrónico de 1.5× (sin gran aumento).
Materiales y métodosSe realizó un estudio de cohorte retrospectivo en pacientes consecutivos con síntomas dispépticos en un centro endoscópico privado dentro del periodo de tiempo comprendido entre enero de 2015 a diciembre de 2016.
ResultadosUn total de 338 pacientes (63±8.4 años, 40% mujeres) fueron inscritos. La prevalencia de infección por H. pylori fue de 10.9% y la incidencia de metaplasia intestinal en el antro y cuerpo gástrico fue de 23.9% y 5.9%, respectivamente. Entre los pacientes con metaplasia intestinal el 65.3% presentó tipo incompleto, 42.7% enfermedad multifocal y un tercio presentó extensión hacia el cuerpo gástrico. Dos pacientes tuvieron displasia de bajo grado. La sensibilidad de la endoscopia con luz blanca fue de 71.2%, con una tasa de falsos negativos de 9.9%. La sensibilidad, especificidad, el valor predictivo positivo, el valor predictivo negativo y la precisión de la imagen de banda estrecha (con crestas azules claras positivas) fue de 85%, 98%, 86.8%, 97.7% y 87.2%, respectivamente.
ConclusiónLa prevalencia de infección por H. pylori y de metaplasia intestinal en pacientes mexicanos dispépticos no fue alta. A través de la valoración de la estructura de la microsuperficie y de signos de crestas azules claras, la imagen de banda estrecha sin zoom óptico tuvo valores predictivos altos para la detección de metaplasia intestinal en pacientes de marco general occidental.
Gastric cancer (GC) is the third leading cause of cancer death worldwide. In most cases, it is detected at an advanced clinical stage and has a poor overall 5-year survival. In 2012, there were 952,000 new cases and 723,000 deaths reported across the world.1–2
Helicobacter pylori (H. pylori) infection in the gastric mucosa causes chronic persistent inflammation involving neutrophils or lymphocytes, and the carcinogenic sequence includes subsequent multiple steps, ranging from chronic atrophic gastritis (CAG), intestinal metaplasia (IM), and dysplasia to cancer.3
CAG and IM are the earliest phenotypic markers in the gastric carcinogenic sequence, and surveillance will depend on histologic confirmation of those lesions. The site, number, and size of the biopsies are factors associated with sampling error. White light endoscopy (WLE) does not clearly visualize such mucosal changes and so the biopsies are taken randomly. The presence of IM and its extension increases the chance of developing GC.4 Intensive surveillance and systematic assessment in such patients may increase the detection of early lesions and diminish the risk of interval GC.5–7
The optical technique, narrow-band imaging (NBI), characterizes the blood vessels and the mucosal surface patterns by illuminating two specific short wavelength lights (blue: 415nm and green: 550nm) through the narrow-band filter. The combination of magnification endoscopy (ME) with NBI (NBI-ME) makes it possible to identify the detailed microvascular pattern and microsurface patterns of the superficial gastric mucosa that correspond to the histology.8–10 The endoscopic sign of the light blue crest (LBC) is reported to show a high positive predictive value (PPV) for diagnosing histologic IM.11 The reported sensitivity, specificity, and diagnostic efficacy of NBI-ME for IM are 89, 93, and 91%, respectively.12,13 The usefulness of the LBC in NBI-ME for the diagnosis of IM was validated in several randomized controlled trials in Asia.14,15 Despite the technologic advance of NBI, in most countries around the world, 1.5x electronic zoom endoscopy, which has a lower magnification capacity than that of the optical ME, is still commonly used in daily practice. Therefore, the aim of our study was to assess the diagnostic efficacy of non-optical zoom NBI to identify IM in Mexican patients with dyspeptic symptom.
Materials and MethodsStudy design and participantsA retrospective cohort study was conducted at a private endoscopy center in Mexico City. Data of consecutive patients that presented with persistent or recurrent symptoms of dyspepsia between January 2015 and December 2016 were retrieved from medical records and endoscopy reports. The data of patients with the following conditions were excluded: gastrointestinal bleeding, perforation, intestinal obstruction, advanced gastric cancer, stenosis, gastric resection, portal hypertension, and allergy to dimethicone. Clinical and demographic data, such as smoking history, drinking habit, family history of gastric cancer, and body mass index (kg/m2) were documented in all the patients.
Endoscopic procedure and definition of findingsPatients fasted for > 8hours before gastroscopy. With continuous drip infusion of 0.9% physiologic saline solution and oxygen administration through nasal prongs at a rate of 3 l/min, propofol sedation was given by an anesthesiologist, according to baseline requirements. Vital signs (blood pressure, heart rate, respiratory rate, body temperature, oxygen saturation) were continuously monitored and recorded.
A single endoscopist (SSC) examined the gastric mucosa, using an EVIS EXERA II system and H-180 gastroscope (Olympus Medical Systems, Tokyo, Japan). Images were taken from the antrum and the corpus to evaluate the performance of endoscopy for diagnosing intestinal metaplasia.
First, the gastric mucosa was observed through conventional white light endoscopy, and the following endoscopic findings were used as indicators for the diagnosis of IM: whitish mucosa, a rough and uneven mucosal surface, a villous appearance, atypical collecting venules (CV), and patchy redness.15
Next, the mucosa was observed through NBI. Microsurface patterns were diagnosed under 1.5x electronic magnification as regular, irregular, and absent, according to the pattern of the crypt epithelium12 or the white opaque substance (WOS).16
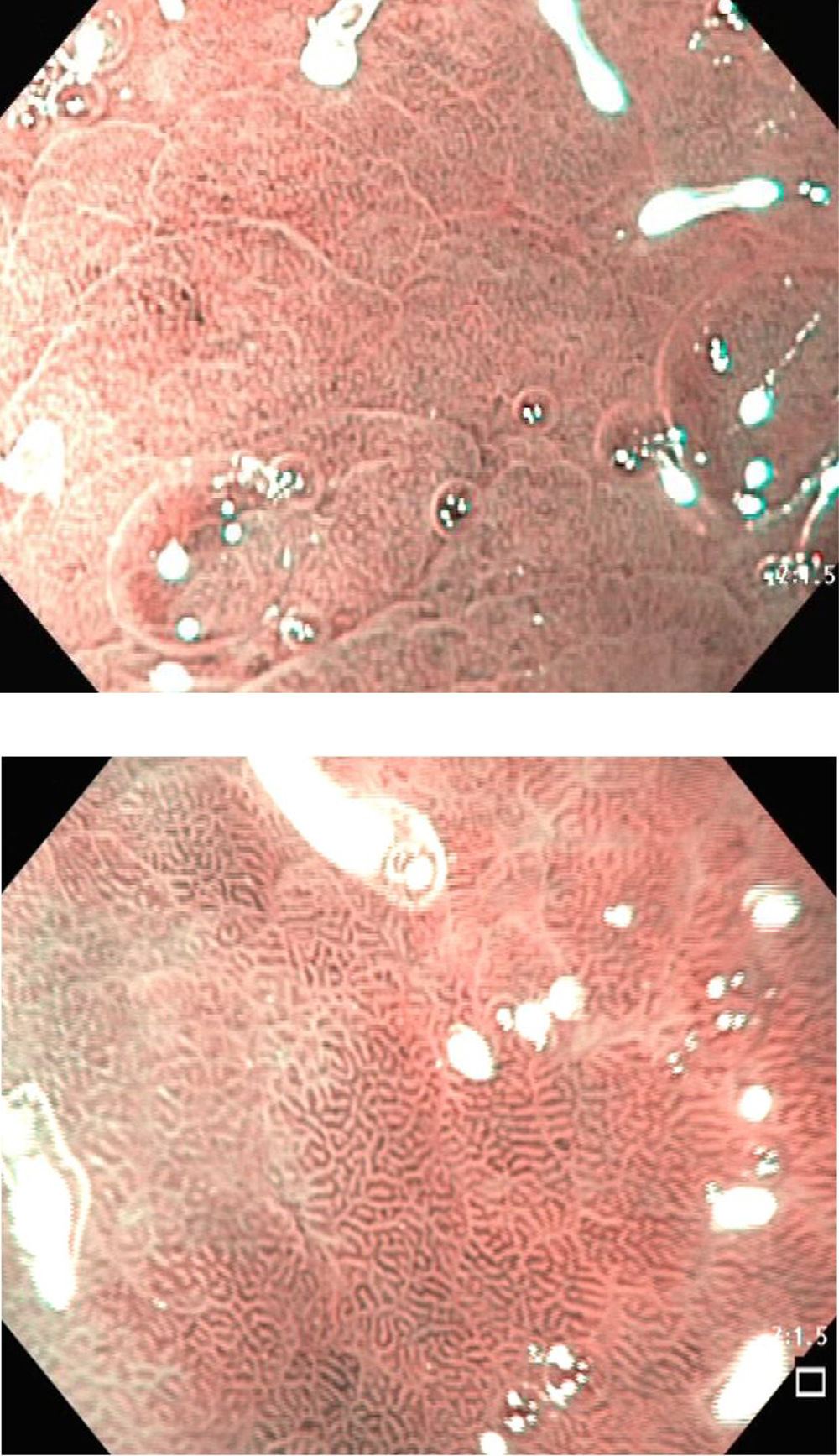
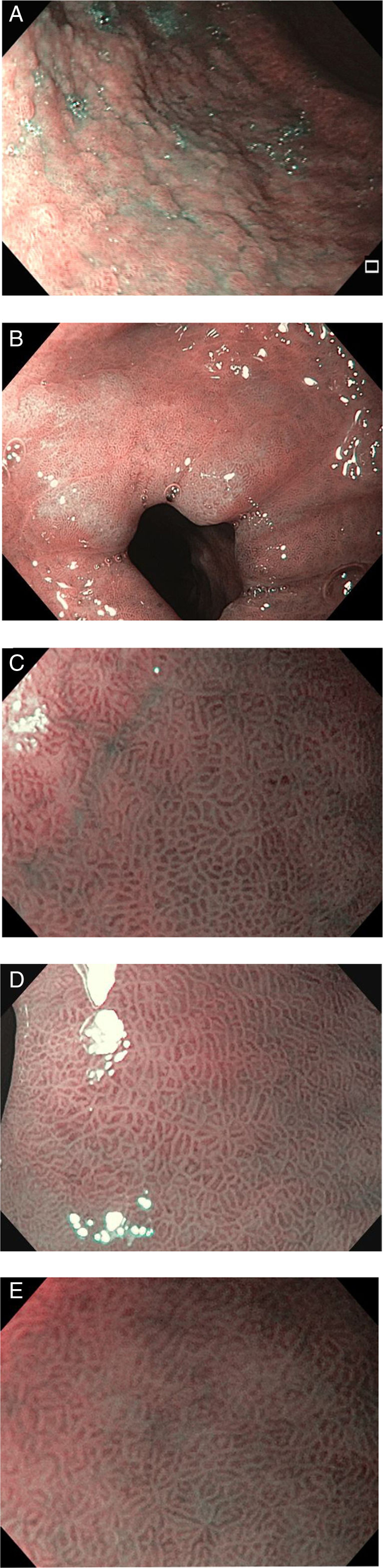
The diagnostic criteria in NBI were:12 1) Non-IM: regular oval-shaped or circular crypts surrounded by vessels with a regular distribution (fig. 1). 2) IM: regular crest/tubulovillous mucosa and regular blood vessels with LBC (fig. 2). The endoscopic sign known as LBC is an irregular whitish-blue area that can be observed on the surface of the gastric epithelium through NBI-ME (magnification endoscopy). Upon the endoscopic finding of IM, targeted biopsies were taken with standard biopsy forceps. In the absence of lesions, the biopsies were performed randomly (2 from the antrum and one from the corpus). The antrum biopsies were placed together in a vial pod (338) in 10% formaldehyde and labeled separately from those of the corpus (338 biopsies).
.")
. A) Nodular mucosa on the gastric corpus. B) irregular whitish-blue area observed through NBI. C-E) The light blue crest (endoscopic sign).")
Hematoxylin and eosin staining was performed. Specimens were also screened for H. pylori infection using a modified 2% Giemsa stain. An expert pathologist (Márquez, ML), trained in gastrointestinal pathology, processed all the mucosal specimens. Neither clinical information nor endoscopic findings were blinded to the pathologist.
The degrees of neutrophil infiltration (activity), mononuclear cell infiltration (inflammation), atrophy, and IM were graded according to the updated Sydney system (normal, mild, moderate, or severe).17,18 Atrophy was defined as the loss of glands with or without metaplasia. The presence of any grade of IM in the biopsy specimen served as the reference standard for the endoscopic diagnosis of IM. IM was sub-classified into incomplete or complete types and focal or multifocal types.19 (fig. 3).
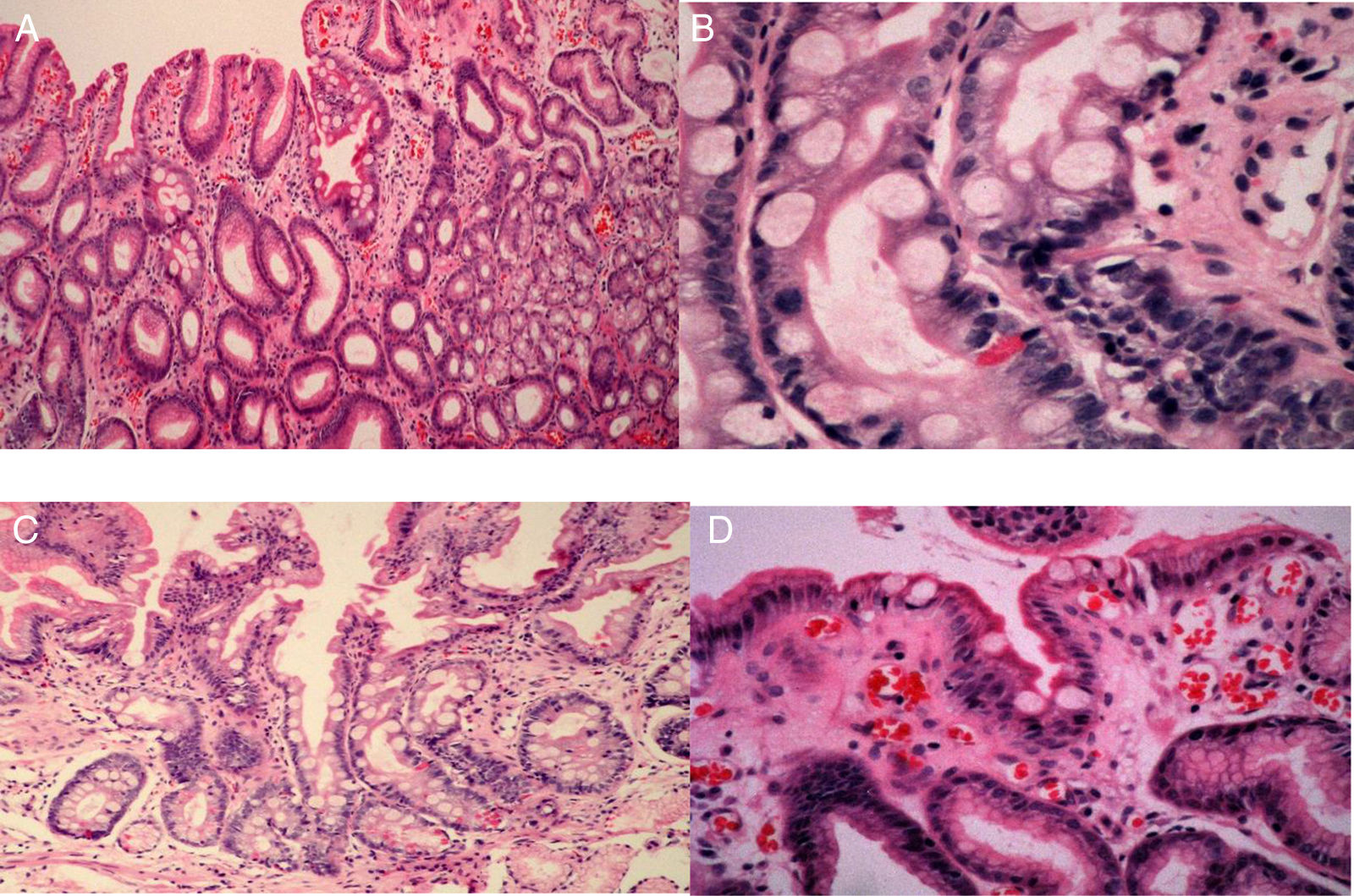
 Focal incomplete intestinal metaplasia: goblet cell (bold arrow), brush border enterocytes (thin arrow), and normal foveolar epithelium (cross). B) Complete intestinal metaplasia: goblet cell (thin arrow), enterocyte (bold arrow), and Paneth cell (short arrow). C) Complete intestinal metaplasia: goblet cell (thin arrow), enterocyte (long arrow), and Paneth cell (wide arrow). D) incomplete intestinal metaplasia: enterocytes (thin arrow), goblet cell (bold arrow), and foveolar epithelium (cross).")
Histologic images of gastric intestinal metaplasia. A) Focal incomplete intestinal metaplasia: goblet cell (bold arrow), brush border enterocytes (thin arrow), and normal foveolar epithelium (cross). B) Complete intestinal metaplasia: goblet cell (thin arrow), enterocyte (bold arrow), and Paneth cell (short arrow). C) Complete intestinal metaplasia: goblet cell (thin arrow), enterocyte (long arrow), and Paneth cell (wide arrow). D) incomplete intestinal metaplasia: enterocytes (thin arrow), goblet cell (bold arrow), and foveolar epithelium (cross).
Complete IM (type I) was characterized by goblet cells spread among the absorptive columnar cells and intercalated between the secretory columnar cells that resemble the gastric foveolar cells or the colorectal cells to a certain extent. The incomplete type was defined by multiple intracytoplasmic mucin droplets of varying sizes and shapes, and the absence of a brush border.18 Focal was defined as the presence of IM in either the antrum or the corpus, and multifocal IM was defined as the presence of IM in both areas.20
Statistical analysisDescriptive statistics were used to calculate frequencies and proportions. The χ2 test was used for categorical variables with a 0.05 significance level. The premalignant lesion detection index was calculated. Diagnostic performance of the LBC for diagnosing IM was estimated. A diagnostic test was performed, calculating the sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), likelihood ratios (LR), diagnostic accuracy, and disease prevalence. The SPSS 19.0 statistics program was used to calculate the values of the variables.
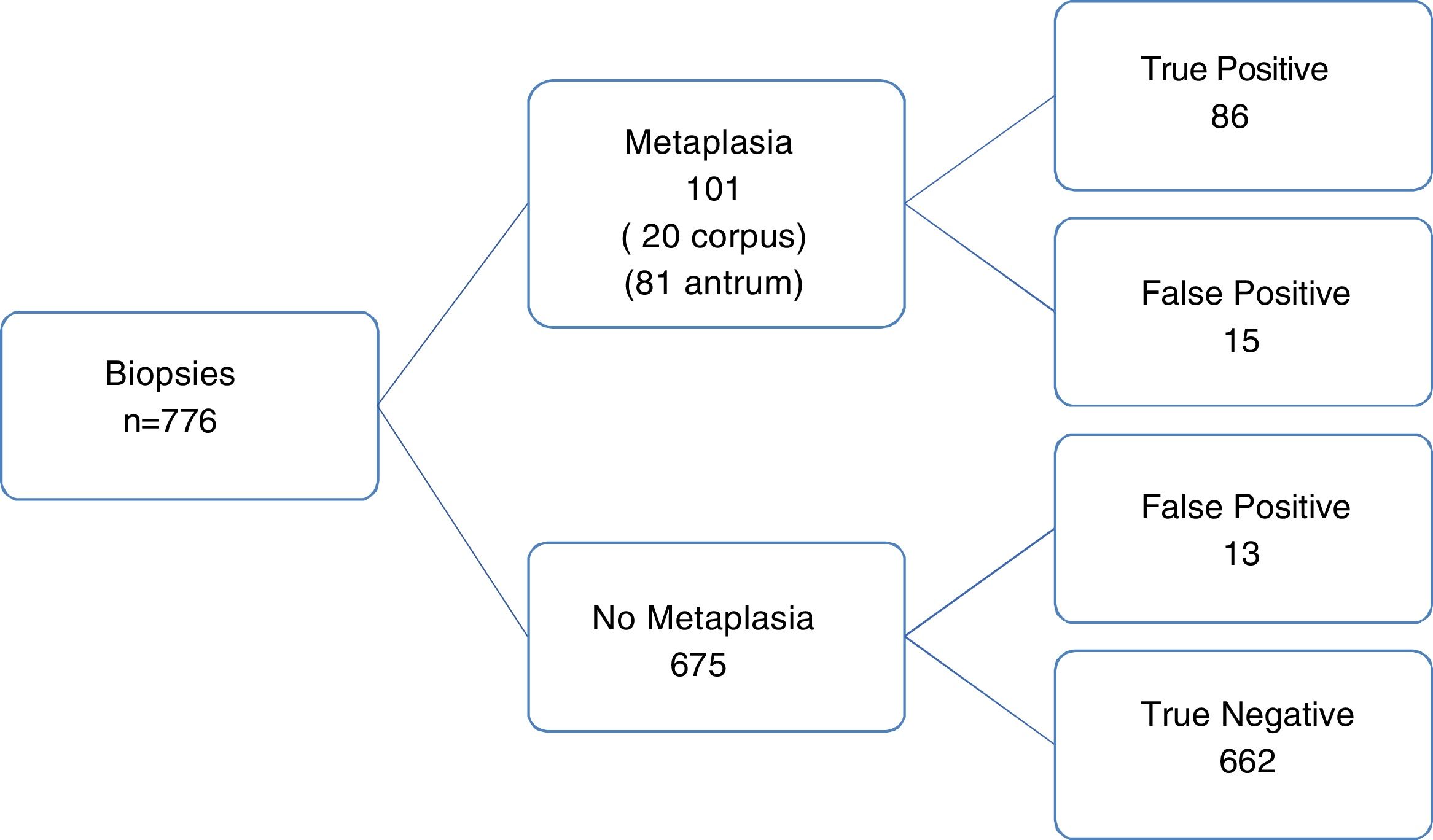
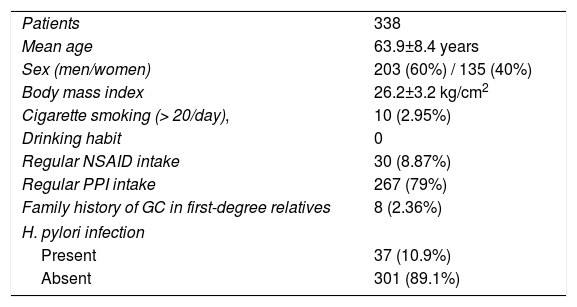
ResultsA total of 338 consecutive patients (776 biopsies) were included in the study. Demographic data are listed in Table 1. All patients had dyspepsia symptoms (age 63.9±8.4 years, 203 men and 135 women, and a mean BMI of 26.2±3.2). Only 8 subjects (2.36%) had a family history of gastric cancer in a first-degree relative.
Demographics of the study participants.
| Patients | 338 |
| Mean age | 63.9±8.4 years |
| Sex (men/women) | 203 (60%) / 135 (40%) |
| Body mass index | 26.2±3.2 kg/cm2 |
| Cigarette smoking (> 20/day), | 10 (2.95%) |
| Drinking habit | 0 |
| Regular NSAID intake | 30 (8.87%) |
| Regular PPI intake | 267 (79%) |
| Family history of GC in first-degree relatives | 8 (2.36%) |
| H. pylori infection | |
| Present | 37 (10.9%) |
| Absent | 301 (89.1%) |
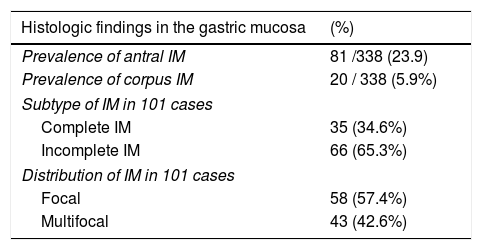
The prevalence of H. pylori infection in the biopsy sample was 10.9% (37/338 patients). The prevalence of IM in the antrum and corpus was 23.9 and 5.9%, respectively (Table 2). IM was incomplete in 65.3% of the patients and multifocal in 42.6% (fig. 1). There were 2 cases of low-grade dysplasia. In 20/81 (24.6%), the metaplasia extended all the way to the gastric corpus. No early gastric cancer was observed during the evaluations of the present study.
Histologic changes in consecutive cases of patients with persistent or recurrent symptoms of dyspepsia.
| Histologic findings in the gastric mucosa | (%) |
|---|---|
| Prevalence of antral IM | 81 /338 (23.9) |
| Prevalence of corpus IM | 20 / 338 (5.9%) |
| Subtype of IM in 101 cases | |
| Complete IM | 35 (34.6%) |
| Incomplete IM | 66 (65.3%) |
| Distribution of IM in 101 cases | |
| Focal | 58 (57.4%) |
| Multifocal | 43 (42.6%) |
The sensitivity of white light endoscopy for IM was 71.2% (72/101 cases), but the false negative rate was 9.9% (66/665 non-metaplastic biopsies).
Sensitivity and specificity, and the PPV and NPV for detecting IM through NBI were 85% (95%CI: 76.69-91.44), 98% (95%CI: 96.73-98.9), 86.8% (95%CI: 79.3-91.9), and 97.7% (95%IC: 96.5-98.60), respectively, and the diagnostic accuracy was 87.2%, with a prevalence rate of 13% (Graph 3). The positive likelihood ratio (LR+) was 44 (95%CI: 26-76) and the subsequent likelihood was 87% (95%CI: 80-92). The likelihood that a patient with a positive test had the disease was ∼ 1 out of 1.2. The negative likelihood ratio (LR-) was 0.15 (95% CI: 0.09-0.24) and the subsequent likelihood was 2% (95%CI: 1-3). The likelihood that a patient with a negative test was healthy was 1 out of 1.0. figure 4.
Discussion and conclusion.")
The prevalence of H. pylori infection and IM in dyspeptic Mexican patients was not high. The endoscopic sign of LBC was found to have high predictive values for the diagnosis of IM, with high likelihood ratios.
Long-standing H. pylori infection causes chronic gastritis and is the main causative factor leading to IM.21 It consists of the metaplastic transformation of the normal gastric epithelium to IM, as a result of genetic and biomolecular alteration in the epithelial cells.22 There is a 4.5 to 9-fold increased risk for IM in patients with H. pylori infection. This premalignant condition can be detected in one out of 4 subjects undergoing an endoscopy.23 Its prevalence in the Western population ranges between 10 and 20%.24
Among detected IM cases, 69.1% were the incomplete type and 40.7% were multifocal. The progression from gastric IM to gastric adenocarcinoma is highly associated with the incomplete type.23,25 A Colombian study that investigated IM distribution and the risk of gastric cancer indicated that patients with IM extending toward the lesser curvature had a 5.7-fold increased risk (95% CI: 1.3-26) and that patients with the diffuse pattern (IM in both the antrum and the corpus) had a 12.2-fold increased risk (95% CI: 2.0-72.9), compared with patients with IM confined to the antrum.19 Those results suggest that, even though the prevalence of H. pylori infection and IM is not high in Mexican patients with dyspeptic symptoms, a certain fraction of patients in our population has a substantial risk for developing gastric cancer (24.6% with extended IM). The primary goal for reducing gastric cancer mortality is early-stage detection and treatment of neoplasias. Therefore, it is of the utmost importance for endoscopists to identify IM and take a biopsy specimen, and for the pathologist to report both the type of IM (complete/incomplete) and its extension.26
In a consecutive case series in Japan, IM was more frequent among H. pylori infected subjects than among non-infected ones (37 versus 2%).27,28 The bacterial infection rate among our cases was very low (11.8%), even lower than the prevalence of IM. This was most likely due to the chronic use of PPIs, the use of a single diagnostic method (histology), and to not evaluating the bacteria in the proximal segments of the stomach. Patients that smoke >20 cigarettes/day are reported to have at a higher risk of developing IM (4.75, 95% CI: 1.33-1.99),22 and the same holds true for patients with the cagA strains.28 In our case series, only 1.95% of the patients reported chronic heavy smoking and only two had focal antral IM. The presence of virulent strains was not evaluated in our study. Therefore, a H. pylori infection test, alone, might not be a useful method to identify patients presenting with IM that is a precancerous condition for gastric cancer in Mexico.
There is an increased risk for developing IM (a 2.6 to 3.5-fold increase; 8% calculated attributable risk) in individuals that have a first-degree relative with gastric cancer.29 The prevalence rate of IM is higher in that population than in controls. The odds ratio reported in a meta-analysis was 1.98 (95% IC: 1.363-2.881).23 The prevalence of subjects with a first-degree relative with GC was very low in our study sample, which could be one explanation for the low prevalence of IM in our study subjects. However, it is possible for a sole H. pylori infection to cause IM in an individual with no family history of gastric cancer.
The importance of surveillance in patients with a high-risk mucosal condition, i.e. atrophy and/or IM, has been a controversial topic. IM regression through H. pylori eradication has not shown sufficiently convincing results. A meta-analysis of 7 studies did not report a significant regression of IM in the antrum (OR: 0.795; 95% CI: 0.587-1.078; p=0-14) or in the corpus (OR: 0.891; 95%CI: 0.633-1.253; p=0.56) after bacterial eradication.30 Shichijo et al.31 indicated that IM was the predictor of gastric cancer development after eradication therapy. There is thought to be a breaking point, or point of no return, within the carcinogenic sequence, at which reversion is not possible. IM probably represents that breaking point, or point of no return, in gastric carcinogenesis.32 Thus, IM diagnosis and the recommendation of surveillance endoscopy are important in those patients, even if H. pylori was not detectable or was eradicated.
The endoscopic finding of IM was first described in 1966 by Takemoto as grayish-white raised lesions scattered on the mucosa of the pyloric antrum and the gastric angle.35 In 2002, Kaminishi et al.34 investigated the diagnostic accuracy of that finding. However, even though the presence of grayish-white elevations was highly specific (98-99%), it had very low sensitivity (6-12), and so they concluded that IM diagnosis should be based on histology and that standard endoscopy was not appropriate for diagnosing IM.
Recently, Fukuda et al.35 included other endoscopic findings of IM through white light endoscopy and used a high-definition video-endoscope, demonstrating a better endoscopic diagnostic performance for IM. In the present study, we used the same endoscopic findings to diagnose IM through white light endoscopy, detecting IM with a sensitivity of 76.5%. Using NBI (the LBC sign), we detected IM with a sensitivity of 85.1%, resulting in an 8.5% increase in the diagnostic yield. Moreover, the false positive rate decreased significantly from 24.5 to 3.9%. NBI contrasts the microvascular architecture and surface structure of the superficial mucosa, and with magnification, allows us to observe the details of the morphologic characteristics of the epithelium.33 In 2012, a reproducible classification of NBI was validated, with accuracy rates of 85 and 90% for the diagnosis of IM and dysplasia, respectively.36 The reported sensitivity was 87% (83-91), specificity was 97% (95-98), LR+ was 27.8 (19-41), and LR- was 0.13 (0.1-0.17) for IM. NBI increased the diagnostic yield more than 10% and achieved a 94% diagnostic efficacy rate.37 In our case series, it had a greater effect on the false positive rate, and the false negative rate was not statistically significant when compared with WLE. Cumulative sensitivity has been reported at 0.86 (95% CI: 0.83-0.89), with a specificity of 0.88 (95% CI: 0.84-0.91), a LR+ of 7.131 (95% CI: 4.39-11.59), a LR- of 0.15 (95% CI: 0.08-0.30), and an area under the Receiver Operating Characteristic (ROC) curve of 0.9482.35 We obtained a sensitivity of 85%, a specificity of 98%, a PPV of 86.8%, and a NPV of 97.7% for detecting IM with the LBC. The likelihood ratios were appropriate. Capturing images according to the systematic screening protocol for the stomach (SSS) assures an objective assessment of the endoscopic finding of IM and its use would enable us to relate the endoscopic findings to clinically relevant outcomes.26
The absence of a tubulovillous mucosal pattern (B pattern) or the LBC can exclude the presence of IM. Therefore, the diagnosis of IM through an endoscopic finding is important, not only for the identification of high-risk patients, but also for excluding low-risk patients from intensive screening and surveillance. LBC originates from the reflection of light on the ciliated structure on the surface of the IM (brush border). The IM epithelium appears turbid, compared with the non-metaplastic mucosa.9,38 Thus, diagnosis of mucosal characteristics through NBI-ME would directly correspond to the histologic changes of the gastric epithelium. High magnification optical zoom endoscopy is not widely used in Western countries, but our results support the feasibility of using non-optical electronic zoom NBI for the diagnosis of IM by detecting the endoscopic sign of LBC to stratify risk in the Mexican patient.
Our study has several limitations. First, due to its retrospective design, the results must be confirmed in a prospective analysis. Second, two biopsy specimens from the antrum were placed together in a vial pod, but evaluated separately from the corpus specimens. Third, the exclusion criteria did not include PPI use (within the past 30 days) for the detection of bacteria. Fourth, the clinical information was not blinded for the pathologist and it may have affected the external validity of the study. And last, the lack of a cap at the tip of the endoscope for fixing the position and obtaining better-quality images made it difficult to observe the capillaries.
In conclusion, the prevalence of IM in the gastric antrum and corpus in patients with persistent symptoms of dyspepsia was 23.9 and 5.9%, respectively. In Mexico, Helicobacter pylori infection was detected in only 10.9%. Through the evaluation of the microsurface structure and the LBC, non-optical zoom NBI showed high predictive values for the diagnosis of antral IM, with significant likelihood ratios, in a Western setting.
Ethical disclosuresProtection of human and animal subjectsThe authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Sobrino-Cossío S, Abdo Francis JM, Emura F, Galvis-García ES, Márquez Rocha ML, Mateos-Pérez G, et al. La eficacia de la imagen de banda estrecha para la detección de metaplasia intestinal en pacientes adultos con síntomas de dispepsia. Revista de Gastroenterología de México. 2018;83:245–252.

