
Adherence to colorectal cancer (CRC) screening is essential for the effectiveness of screening programs. Even though organized screening programs can improve the quality of the process and adherence, there are still challenges to overcome. The aim of the present study, in which we implemented a biennial organized screening program for CRC, was to describe adherence and participation patterns.
Materials and methodsA longitudinal, descriptive study was conducted, in which a team of trained patient navigators carried out interventions, with reminders via cellphone communication, to follow a cohort of 301 subjects eligible for CRC screening, utilizing a fecal immunochemical test (FIT). All the follow-up subjects received a FIT kit.
ResultsA total of 747 cellphone calls were made and divided into three interventions. From the initial cohort, 126 subjects completed their biennial screening process through the FIT, indicating a consistent adherence rate of 41.8% to our program. The participation patterns were: 126 consistent participants (41.8%), 160 inconsistent participants (53.2%), and 15 participants that were never contacted (5%).
ConclusionsIn conclusion, our study underlines the importance of organized screening programs in the early detection of CRC. The implementation of follow-up interventions, through reminders and the training of patient navigators, can improve adherence, but there is a need for examining new strategies, to overcome barriers to communication via cellphone.
La adherencia al tamizaje del cáncer colorrectal (CCR) es esencial para la efectividad de los programas de escrutinio. A pesar de que los programas de tamizaje organizado pueden mejorar la calidad del proceso y la adherencia, aún hay desafíos para lograrlo. En este estudio, implementamos un programa bienal de tamizaje organizado para CCR con el objetivo de describir la adherencia y los patrones de participación.
Materiales y métodosSe realizó un estudio longitudinal y descriptivo en el que un equipo de navegadores de pacientes capacitados realizó intervenciones con recordatorios mediante llamadas telefónicas para dar seguimiento a una cohorte de 301 sujetos elegibles para el tamizaje de CCR mediante una prueba de inmunoquímica fecal (FIT). Todos los participantes que cumplieron con su seguimiento recibieron un Kit FIT.
ResultadosSe realizaron 747 llamadas telefónicas divididas en tres intervenciones. De la cohorte inicial, 126 sujetos completaron su proceso de tamizaje bienal mediante FIT, lo que indica una adherencia consistente del 41.8% a nuestro programa. Los patrones de participación fueron 126 participantes consistentes (41.8%), 160 inconsistentes (53.2%) y 15 nunca atendidos (5%).
ConclusionesEn conclusión, nuestro estudio resalta la importancia de los programas de tamizaje organizado en la detección temprana del cáncer colorrectal. La implementación de intervenciones de seguimiento mediante recordatorios y la capacitación de navegadores de pacientes, puede lograr mejoras en la adherencia, sin embargo, es necesario explorar nuevas estrategias para superar las barreras en la comunicación telefónica.
Colorectal cancer (CRC) is one of the main causes of death from cancer worldwide. It is the second most common cancer in women and the third in men. Over the past two decades, an increase in the incidence of CRC in middle and low-income countries has been observed due to factors such as the westernization of diets, obesity, smoking, a sedentary lifestyle, population aging, and the lack of organized screening programs. In contrast, developed countries have achieved a decrease in CRC-related mortality thanks to prevention and early detection through screening programs implemented since the 1990s.1
For the year 2030, a 60% increase in the global burden of CRC is expected, underlining the need to prioritize primary prevention and early detection, especially in low and middle-income countries.2
Although 60–70% of the cases of CRC are diagnosed at late stages of the disease, secondary prevention through screening tests is an efficacious tool for reducing the mortality rate.3 The majority of the international guidelines recommend starting screening from 45 or 50 years of age, in persons with an average risk for developing CRC.4 The different screening methods include the guaiac fecal occult blood test (FOBT), the fecal immunochemical test (FIT), stool DNA testing, flexible sigmoidoscopy, colonoscopy, and computed tomography colonography.5
The implementation of organized screening programs is an effective strategy for reducing the incidence and mortality of CRC. These programs also offer important benefits, such as increasing adherence to screening, improving the quality of the services, and reducing costs. They also provide clear and precise information on the screening options available to patients, which can reduce the anxiety and stress related to the process. Likewise, follow-up and care after screening are essential for guaranteeing the early detection and effective treatment of CRC.6
Adherence to screening programs varies significantly worldwide, underlining the importance of implementing strategies to improve the participation of the population. In the United States, adherence rates have been reported at between 23 and 53%,7,8whereas higher adherence rates have been achieved through organized screening programs.9 Therefore, continuous efforts are needed to measure and optimize adherence to screening. Personalized strategies, such as interactive reminders or patient navigators, should also be considered, to improve participation in the population.10,11
Patient navigators, also known as healthcare facilitators, are professionals trained to guide patients and direct them through all the screening steps. This has been shown to be an effective method for increasing adherence rates, not only in CRC screening, but also in other types of cancer.12 The measurement of longitudinal adherence and participation patterns is essential for identifying areas of opportunity and factors that limit follow-up, to then develop interventions and strategies for reducing losses in the screening process.
The aim of our study was to implement an organized screening program for CRC, using an intervention team, for the purpose of describing biennial adherence to the program and the corresponding participation patterns.
MethodologyDesignA longitudinal, descriptive study was conducted, in which a biennial organized screening program for CRC was designed, utilizing the fecal immunochemistry test (FIT). The participants were selected through convenience sampling.
Subject recruitmentSubjects over 50 years of age and residents of Veracruz, Mexico, that were considered to have an average risk for developing CRC and who expressed an interest in participating in the screening program, were recruited between January and June 2019. Participants were selected by means of conferences on CRC directed at workers and academic personnel from different dependencies of the Universidad Veracruzana. The exclusion criteria were age above 80 years and having a high risk for CRC, terminal or decompensated illnesses, or signs of recent bleeding. The eligible individuals were scheduled to be seen by a team of physicians trained in screening for CRC.
Patient interviewAll participants were personally interviewed by physicians trained in CRC screening, to provide information on prevalence, etiology, adenoma-carcinoma sequence, screening methods, recommended time intervals, and challenges regarding adherence. Likewise, a written questionnaire was applied to collect information on age, sex, body mass index (BMI), alcoholism, smoking, physical activity, and nonsteroidal anti-inflammatory drug (NSAID) use.
Detection of occult blood in stool through the fecal immunochemical testTo detect fecal occult blood, the participants were given a screening kit that included a container for collecting the sample, an instruction pamphlet, and a quantitative FIT (OC FIT-CHEK®, Polymedco, Cortlandt Manor, NY, USA). The participants were asked to collect the stool sample and return the FIT kit within the next three days. All samples were processed by a central laboratory utilizing an automated testing method recommended by the manufacturer (Eiken Chemical, Tokyo, Japan). To define an abnormal FIT result, and then refer those patients to colonoscopy, a cutoff point >100 ng of hemoglobin/mL of buffer ( = 20 μg of hemoglobin/g from stool) was used. The patients with abnormal results were contacted via telephone to personally receive their results and continue with the next step of screening. Colonoscopies were performed by an experienced, certified endoscopist. Polypectomy with biopsy was carried out, when indicated, and the results were reviewed by a pathologist with expertise in the gastrointestinal tract. Within the study methodology, specific time periods were established to manage positive results and schedule the colonoscopies. One week after a positive result was obtained, direct contact was made with the patient. Colonoscopy was then scheduled and performed, no later than one month after having informed the patient that the procedure was necessary. All the patients received their results and follow-up recommendations from the general physician. The patients with adenomas were referred to the gastroenterology service for individualized medical and endoscopic follow-up.
Patient navigatorsTo improve CRC screening program adherence, an intervention was implemented that included the training of a team of five patient navigators, who were pre-graduate physicians. The training was carried out by a gastroenterologist, who gave specialized talks on different aspects related to CRC.
The talks included the themes of risk assessment for CRC, the different screening methods available, the use of effective communication tools, and intercultural learning. The aim of the training was to provide the patient navigators with the knowledge necessary for offering the screening program participant comprehensive and quality advice.
In addition to the training, as part of the intervention, a detailed telephone call script was designed and used by the patient navigators to contact the participants of the 2019 screening program and invite them to participate again in the 2021 program, within the time frame of January to June.
Cellphone call patternsThe cellphone call patterns were registered according to the response obtained as “answered”, “rang but no answer”, “outside of the area of cellphone service”, “call went to voicemail”, “wrong number”, “nonexistent number”, “participant not interested”, and “participant no longer living”. Likewise, the biennial participation patterns were registered, identifying participant adherence as follows: “consistent adherence” (for those that attended the biennial screening), “inconsistent (late) adherence”, and “no adherence”.
The participants that attended their 2021 biennial screening round received personalized attention from their assigned navigator, who once again gave them detailed information about CRC and the different screening methods available and answered their questions. At the end of the interview, the general physician explained the sample collection process and provided additional feedback on the aspects previously discussed. The remainder of the screening process was carried out with the same methodology utilized during the first screening round.
Longitudinal adherence: participation patternsThe stratification of attendance to the biennial screening round was calculated, considering the previous participation of the individuals. In addition, the different participation permutations were described (consistent, inconsistent, nonexistent).13 To calculate biennial adherence, only the participants that concluded the screening process through the FIT in the two consecutive years (consistent participants) were considered. The formula employed for calculating consistent biennial adherence was: (number of subjects that met the criterion)/(total number of initial participants).
Statistical analysisData distribution was evaluated using the Kolmogorov-Smirnov test. The numerical variables were reported as median and interquartile range, and the categorical variables were expressed as frequency and percentage. The consistent adherence rate was calculated by dividing the number of participants with consistent biennial adherence by the total of initial participants. The groups were compared using the Student’s t test or the Wilcoxon test, as applicable. The chi-square test or Fisher’s exact test were utilized for the categorical variables. The analysis was carried out using the SPSS (IBM, Armonk, NY, USA) V.24 program.
Ethical considerationsThis protocol was evaluated and accepted by the scientific ethics committee with folio llMB-2019-03 and was carried out in accordance with the principles of the Declaration of Helsinki. All the subjects participated voluntarily, free of charge, and signed statements of informed consent, in which the procedure and risks and benefits of the study were explained. The results were also explained and sent to the participants, either by email or in printed form. The subjects with abnormal results were referred to the corresponding health services for diagnosis or early treatment. All tests were carried out free of charge for all the study participants.
ResultsInitial 2019 cohortIn 2019, a total of 301 subjects, 73.4% of whom were women, arrived at our institution. They received a FIT kit and were personally interviewed by the corresponding patient navigator. The median age of the participants was 61 years, with a range of 55–68 years. Of the participants, 277 (92%) returned the FIT kit exactly as requested. Upon analyzing the returned FIT kits, 13 (4.3%) were found to be positive. Eleven colonoscopies were consequently performed, revealing adenoma in 36.3% of the cases. A description of the evaluation results of the adenomas found in the patients follows below.
Patient 1: A 62-year-old man. Four adenomas with low-grade dysplasia were identified, located in different segments of the colon, including the ascending colon, transverse colon, descending colon, and sigmoid colon. In addition, the presence of mild chronic colitis was observed, accompanied by marked eosinophilia, registering up to 43 eosinophils in a high-power field.
Patient 2: A 65-year-old woman. Three tubular adenomas with low-grade dysplasia in the cecum, transverse colon, and descending colon were found.
Patients 3 and 4: A 57-year-old woman and a 68-year-old woman, respectively. Both presented with a single adenoma, with low-grade dysplasia, in the descending colon.
Follow-up in 2021: interventions carried outIn 2021, the initial cohort was followed, excluding the patients that did not return their FIT kit. The remaining 277 participants, 72.8% of whom were women, were contacted by cellphone. Three interventions via cellphone were carried out, with a maximum of 3 calls attempted per subject, with a one-week interval between calls. In the first intervention, a total of 396 calls were made, establishing effective contact with 179 subjects (45.2%). Of those contacts, a FIT kit was given to 93 patients, representing 52% of the contacts and 23.4% of the calls made. In the second intervention, 191 calls were made, achieving successful contact with 84 subjects (44%). Of those successful contacts, a FIT kit was given to 31 patients, the equivalent of 37% of the subjects contacted and 16.2% of the calls made. Lastly, in the third and final intervention, 160 calls were made, achieving effective contact with 24 subjects (15%). A FIT kit was given to eight patients, representing 33.4% of the subjects contacted and 5% of the calls made.
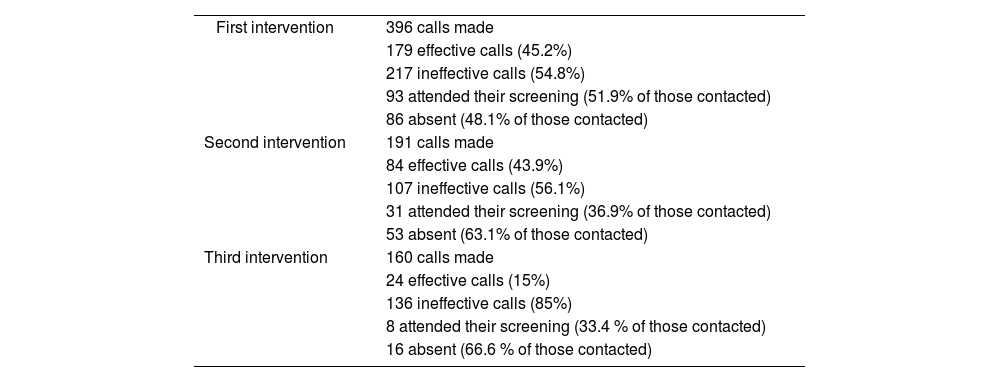
In summary, a total of 747 calls were made throughout the study, with a 38.4% success rate (287 effective calls) and a 61.6% failure rate (460 ineffective calls). The ineffective call patterns were distributed as follows: 34.1% of the calls were not answered by the recipient, 30.6% calls were sent to voicemail, 25.2% calls could not be connected because the recipient was out of the area of cellphone service, 5.8% calls corresponded to a nonexistent number, 2.8% calls were to a wrong number, 0.6% of the recipients were not interested in participating in the study, and 0.6% of the recipients had already died. Table 1 summarizes those findings.
Implementation of the interventions carried out by an intervention team through telephone reminders, to provide follow-up to subjects participating in an organized screening program for colorectal cancer.
| First intervention | 396 calls made |
| 179 effective calls (45.2%) | |
| 217 ineffective calls (54.8%) | |
| 93 attended their screening (51.9% of those contacted) | |
| 86 absent (48.1% of those contacted) | |
| Second intervention | 191 calls made |
| 84 effective calls (43.9%) | |
| 107 ineffective calls (56.1%) | |
| 31 attended their screening (36.9% of those contacted) | |
| 53 absent (63.1% of those contacted) | |
| Third intervention | 160 calls made |
| 24 effective calls (15%) | |
| 136 ineffective calls (85%) | |
| 8 attended their screening (33.4 % of those contacted) | |
| 16 absent (66.6 % of those contacted) |
The intervention consisted of making up to three calls per subject, with a one-week interval between each round of calls. Calls were registered as effective or ineffective. An effective call was one in which the participant was directly contacted and informed about the study. An ineffective call was one in which no communication with the participant was made.
Of the 277 subjects eligible for undergoing the biennial screening, 199 (74.8%) were contacted. Of those subjects, 143 came to our institution to pick up their FIT kit and 126 (88.1%) returned it.
According to the previous participation of the eligible subjects (n = 277), 45.5% (n = 126) participated again in the 2021 screening program. Upon analyzing the different attendance permutations of the initial cohort (n = 301), the following results were obtained: 41.8% (n = 126) of the subjects attended the two screening rounds, 51.2% (n = 154) only attended the first screening round, 2% (n = 6) only attended the second screening round, and 5% (n = 15) did not attend either of the screening rounds.
Regarding the attendance patterns, 126 subjects (41.8%) maintained consistent attendance in the two screening rounds, whereas 160 subjects (53.2%) presented with inconsistent attendance (attending one screening round but not the other). In addition, 15 subjects (5%) were identified that did not attend either screening round.
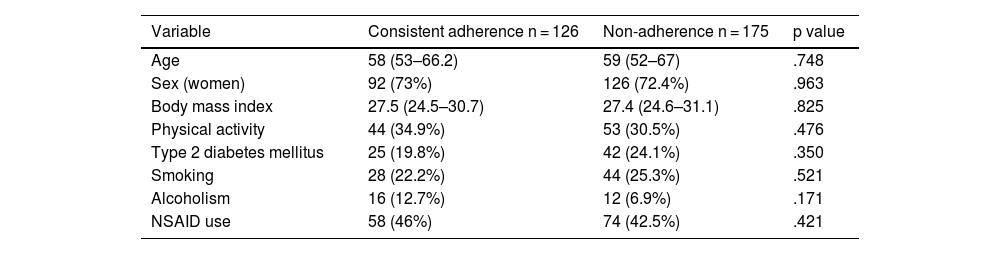
Upon concluding the study, of the 301 initial subjects, a total of 126 successfully completed their biennial screening with a FIT, resulting in a consistent adherence rate of 41.8%. Table 2 shows the epidemiologic characteristics of participants with adherence and nonadherence.
Epidemiologic characteristics of the subjects with consistent adherence and non-adherence to an organized screening program for CRC through the fecal immunochemistry test (FIT).
| Variable | Consistent adherence n = 126 | Non-adherence n = 175 | p value |
|---|---|---|---|
| Age | 58 (53–66.2) | 59 (52–67) | .748 |
| Sex (women) | 92 (73%) | 126 (72.4%) | .963 |
| Body mass index | 27.5 (24.5–30.7) | 27.4 (24.6–31.1) | .825 |
| Physical activity | 44 (34.9%) | 53 (30.5%) | .476 |
| Type 2 diabetes mellitus | 25 (19.8%) | 42 (24.1%) | .350 |
| Smoking | 28 (22.2%) | 44 (25.3%) | .521 |
| Alcoholism | 16 (12.7%) | 12 (6.9%) | .171 |
| NSAID use | 58 (46%) | 74 (42.5%) | .421 |
The numerical values were reported as median with interquartile range and the categorical variables as frequency and percentage. The comparison of the numerical variables was carried out using the Student’s t test or Wilcoxon test, according to correspondence with the continuous variables. Regarding the categorical variables, the chi-square test or Fisher’s exact test were used. Consistent adherence was considered if two consecutive screening rounds were completed, and nonadherence was considered if there was inconsistent adherence or no adherence at all.
CRC is one of the main causes of cancer-related deaths worldwide. Efficient screening programs play an essential role in the early detection of CRC and a decrease in the mortality rate associated with the disease. However, adherence to screening is a crucial factor in maintaining the effectiveness of these programs. Despite the advances achieved, there are still under-studied barriers that limit the consequent participation in the target population.
In the present study, the implementation of an organized screening program based on the FIT is described. Biennial adherence of the participants in the program was evaluated, along with participation patterns. In addition, interventions were implemented, such as patient navigator training and telephone reminders, aimed at improving adherence.
Organized screening is carried out within a framework of comprehensive healthcare systems, with the goal of providing a longitudinal follow-up to participants and promoting persistent adherence. In contrast, opportunistic screening is generally carried out as part of a routine medical check-up by professionals, without a long-term systematic follow-up. Previous studies have shown that organized screening programs are associated with greater adherence to and improvements in the screening process.6
Some of the techniques for improving adherence to screening programs include the training of patient navigators, healthcare via telephone, and the use of culturally appropriate techniques to improve knowledge about CRC.14 In addition, the sending of reminders by means of telephone calls, emails, or letters is an effective, efficient, and economic way to improve program adherence rates.5,6,14–16
The importance of an awareness of the communication challenge in the screening program context stands out. Despite numerous attempts to contact patients through cellphone calls and the participation of patient navigators, diverse difficulties have been found, such as unanswered calls, calls sent to voicemail, incorrect numbers, or phones out of areas of cellphone service. These barriers can influence the lack of notification and effective invitation to the participants. One hypothesis suggests that this problem can be related to the insecurity and harassment that people have, with respect to calls from numbers they do not recognize. This finding is highly relevant and can be considered a starting point for reflecting on the need to develop alternative strategies in Mexico, where the traditional postal service is not efficient and cellphone calls appear to be ineffective.
A possible solution proposal for addressing the abovementioned communication challenges could be the implementation of text messages through mobile applications, such as WhatsApp or other similar platforms. This type of alternative could be a more accessible and less intrusive means of communication, overcoming the barriers associated with telephone calls, thus contributing to improving the notification and participation of individuals in the screening program.11,17
Screening programs for CRC utilizing the guaiac FOBT have reported adherence rates that vary from 38 to 45%, whereas programs with the FIT have reported rates between 38 and 53%.8 In our first pilot screening program for CRC based on the FIT in Veracruz,18 adherence was 35.8% at the biennial follow-up but we achieved adherence of 41.8% in this second program, which could be due to the higher number of interventions we carried out, as well as the educational information we provided the patients with during their initial screening.
Screening for the early detection of CRC is of the utmost importance, but there are different barriers that limit adherence to these programs. Among them are the lack of adequate education of the patient about the disease and its prevention; insufficient information provided by healthcare professionals; internal factors, such as patient knowledge, attitudes, and emotions; intercultural aspects, such as machismo; and fear of and aversion to the procedure.19 There are also external factors, such as the lack of access to healthcare services, the quality of the medical attention received, and language barriers, which can also limit adherence.20–23
In their study evaluating the viability of CRC screening in Uruguay utilizing the FIT, Fenocchi et al. reported that 90% of the patients returned their samples for screening, a result coinciding with our study, in which 88–92% of the participants returned their FIT in the two screening rounds.24 This suggests a high acceptance of the screening program and the detection test in the two populations.
Lastly, the participation patterns in our population were similar to those reported in other populations: consistent participation in all rounds; inconsistent participation, in which participants only attended certain rounds; and no participation on the part of patients that could never be contacted.13 The identification of sociodemographic risk factors that limit screening will enable the detection of patients that do not adhere to the recommendations, and provide them with support, education, and additional motivation to increase adherence.
Our study has methodological limitations that impede the generalization of our results to other populations or contexts. Regarding some of the specific program data, it should be mentioned that in the second screening round of 2021, only 277 of the 301 individuals belonging to the original cohort were contacted. This decision was made in an attempt to optimize efficiency in terms of cost-benefit, given the limited availability of the FITs and the fact that the uncontacted individuals did not return their tests during the first screening round, resulting in ineffective use of institutional resources. Even though the four individuals diagnosed with adenomas could have been left out of the second screening round because of their need for a different type of follow-up, we opted to include them, evaluating the relevance of the data associated with their continued participation. Other limitations include the fact that the participants were selected from an urban university zone, utilizing nonrandomized sampling, which can produce selection bias. In addition, the recruited subjects were above 50 years of age, with an average risk for CRC, which could limit the applicability of the results to other groups. The recording of clinical variables was based on a written questionnaire and a personalized interview, which could have introduced response bias. Also of importance is the fact that our sample was limited to a single year (2019), which might not have been representative of the adherence and participation rates in other years. Therefore, additional studies are needed that address these limitations, to better understand the effectiveness of screening for CRC and its implementation in different contexts.
ConclusionsOur study underlines the relevance of organized screening programs for the early detection of CRC. Significant challenges to adherence, demonstrated by a sustained participation of 41.8% were identified. This figure emphasizes the need, not only to implement different strategies that could modify participation patterns, such as reminders or patient education, but also to analyze the factors that limit adherence to screening, to then develop strategies that optimize the process of screening for CRC.
Financial disclosureNo financial support was received in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.

