Introduction
Functional heartburn (FH) is a subgroup of nonerosive reflux disease consisting of patients with esophageal acid exposure within the physiological range in addition to normal endoscopy.1 The Rome committee has defined FH as an episodic retrosternal burning in the absence of pathological gastro-esophageal reflux (GER), motility disorders or structural explanation. Therefore, pH monitoring, endoscopy and/or motility studies are needed in the evaluation of patients. The Rome II Modular Questionnaire has been translated into Spanish-Mexico and heartburn was present in 35.5% in a volunteer study2 in contrast to 19.6% in a community-based study.3 However, in these populations GER was not ruled out to be able to diagnose FH as precluded by the Rome II criteria.4
On the other hand, heartburn is considered a highly specific symptom of GER,5 but there have been no studies to understand the significance of this symptom in Mexico. In addition, GER defined by pathological acid exposure has been reported in 18.5% of patients with functional dyspepsia not reporting heartburn.6
Therefore we sought to explore the frequency of GER in patients reporting heartburn according to the Rome II Modular Questionnaire in Spanish-México and whether the presence of GER in non heartburn patients is related to the reporting of dyspepsia.
Methods
We reviewed a series of patients who consulted a gastroenterology clinic in a private medicine setting in Mexico City. Patients that answered the Rome II Modular Questionnaire in Spanish-Mexico as part of their consultation and that were tested with upper endoscopy and/or 48-hour esophageal pH monitoring with BRAVOTM capsule were included. Those with a normal upper endoscopy without a pH monitoring to rule out GER were excluded. Heartburn was defined as the presence of burning pain or discomfort in the chest, at least once a week during the previous 3 months in the absence of any difficulty swallowing.4 Patients not fulfilling the above criteria were considered as non-heartburn. Clinical manifestations in the non-heartburn during the previous 3 months were also analyzed. These included globus (feeling a lump in their throat when not swallowing); chest pain; dysphagia (difficulty after swallowing solid or liquids, sticking in the chest or passing down abnormally); belching; vomiting (at least 3 episodes on separate days/week); dyspepsia (discomfort/pain centered in the upper abdomen, above the belly button or pit of the stomach) abdominal discomfort/pain in those without dyspepsia and irritable bowel syndrome (IBS).4
GER was considered positive in the presence of a De-Meester score higher than 14.7 during the 48-hour pH monitoring, or if the endoscopic examination revealed erosive esophagitis according to the Los Angeles classification and/or Barrett's confirmed by the presence of goblet cells in the biopsies.5,7
Variables were analyzed by the Student's t test and X2 when appropriate. A p < 0.05 was considered significant.
Results
Forty patients 44.5 ± 2.5 years old, 25(62.5%) female and body mass index (BMI): 25.5 ± 0.8 kg/m2, were included. Heartburn was reported by 16 (40.0%) of them. There were no differences in BMI (25.5 ± 1.5 kg/m2vs. 25.5 ± 0.9 kg/m2, p = 0.097) and gender distribution (F%: 62.5 vs. 62.5%, p = 1.000) between the heartburn and the non-heartburn groups but there was a trend to a younger age among the first ones (38.4 ± 2.8 vs. 47.8 ± 3.3, p = 0.071).
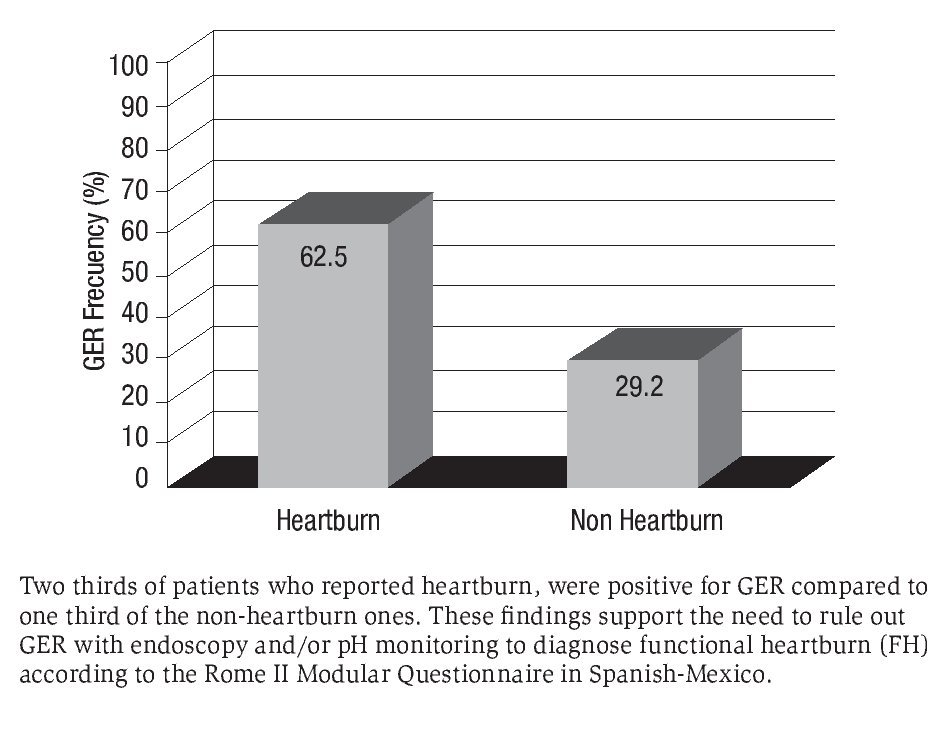
GER was investigated by using upper endoscopies in 90.0% and 48-hour esophageal pH monitoring in 10.0%. Accordingly, GER was present in two thirds of those with heartburn and its frequency was double than that in the nonheartburn ones (p = 0.037) (Figure 1). Findings confirming GER in patients with heartburn were (n): 6 grade A erosive esophagitis, 1 grade B and 3 Barrett's; while in the non-heartburn group: 3 grade A erosive esophagitis, 1 grade B, 1 Barrett's and positive 48-hour esophageal pH monitoring in 2. Based on the above data, 6/16 (37.5%) of those reporting heartburn had FH. Therefore, the real prevalence of FH in our study population was (6/40)15%.
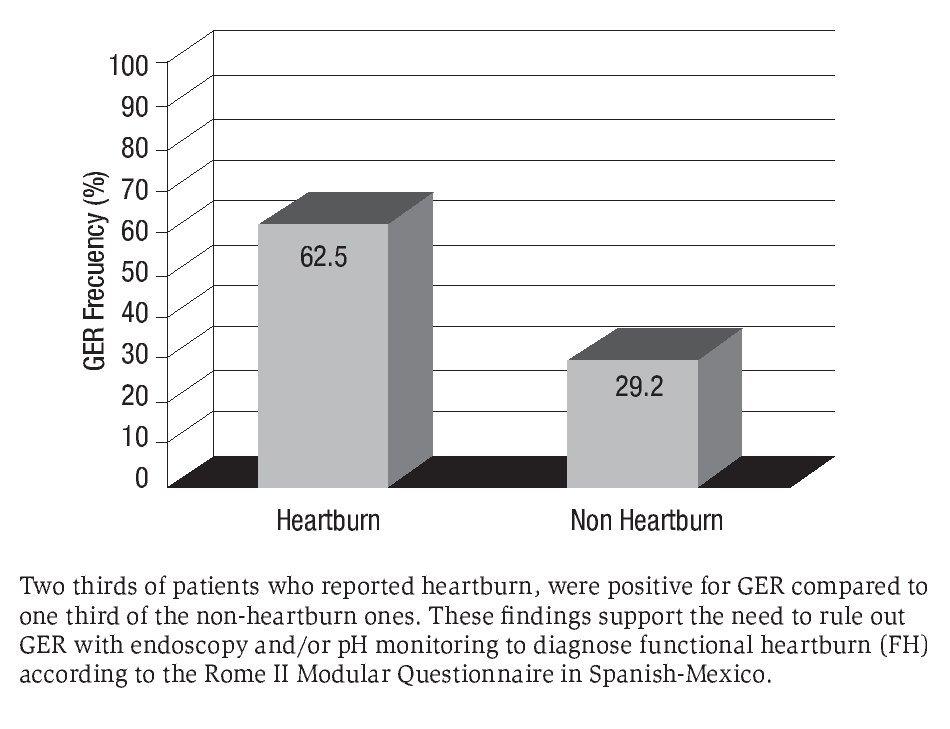
Figure 1. Frequency of GER in patients with and without heartburn according to the Rome II Modular Questionnaire in Spanish-Mexico.
In addition, there were no differences in age, gender and BMI within the heartburn and nonheartburn groups when compared according to the presence or absence of GER (data not shown).
Finally, the clinical manifestations among the 7 non heartburn patients with GER were (n), globus: 1, chest pain: 1, dyspepsia: 3 and abdominal pain: 2. Belching was present in 2 of those with dyspepsia and neither one reported dysphagia, vomiting, or IBS.
Discussion
In the current study among patients that reported heartburn by using the Rome II Modular Questionnaire in Spanish-Mexico validated for that population, 62.5% had GER by endoscopy and/or esophageal pH monitoring compared to 29.2% of those patients not reporting heartburn. Independently of the significant difference in GER between the groups, it is important to note that two thirds of those reporting heartburn were positive for GER. Accordingly; the frequency of FH was 37.5% suggesting that the real prevalence of this disorder in our population would be 1/3 of heartburn reporting. In fact, heartburn is considered a highly specific symptom for GER disease,5 therefore according to the Rome II criteria and the more recent Rome III, GER must be ruled out by pH monitoring and/or endoscopy to diagnose FH in Mexico.4,8
Cultural factors may influence the presentation of symptoms and also the interpretation by physicians. Drossman and Weinland9 recommended that diagnostic criteria and clinical questionnaires be standardized and have achieved adequate cross-cultural validation to correctly identify and compare pattern of illness particularly in functional gastrointestinal disorders. Reported symptoms must fit into the defined criteria to reliably achieve a consistent diagnosis.9 Although the Rome II Modular Questionnaire has been translated and validated into Spanish in Mexico,2 the meaning of heartburn by this questionnaire in the Mexican population had not been previously analyzed. Our findings support the knowledge that in patients reporting heartburn by this questionnaire in Mexico, GER must be ruled out to be able to diagnose FH as precluded by the Rome II criteria.4
On the other hand, an important subset of the non-heartburn patients positive for GER reported dyspepsia symptoms. Our findings are in agreement with those by Tack et al,6 that reported the presence of pathological esophageal acid exposure in a subset of heartburn negative functional dyspepsia patients, characterized by a higher prevalence of epigastric pain. These data also support the need to exclude GER to diagnose functional dyspepsia according to Rome II criteria in Spanish-Mexico as well as the use of empirical treatment for GER with proton pump inhibitors, in patients consulting for functional dyspepsia.
In conclusion, at least two thirds of patients reporting heartburn by the Rome II Modular Questionnaire in Spanish-Mexico, have GER. Therefore, GER must be ruled out to diagnose FH thus proving the concept in the Mexican population in Spanish as precluded by Rome II. Also, a subset of non-heartburn patients with GER in our population, have symptoms of dyspepsia, similar to what has been previously reported by others. The current findings are preliminary and need to be confirmed in larger studies as well as by using the Rome III Questionnaire in Spanish which is currently under translation and validation in a multinational effort in Latin America.10
Correspondence:
Dr. Max Schmulson W.
Laboratorio de Hígado, Páncreas y Motilidad (HIPAM), Departamento de Medicina Experimental, Facultad de Medicina-Universidad Nacional Autónoma de México (UNAM). Hospital General de México.
Dr. Balmis #148. Col. Doctores, C.P.06726. México D.F. México.
Phone number: 52-5556232673, fax: 52-5556232669.
E-mail: maxjulio@avantel.net.
Fecha de recibido: 27 febrero 2009
* Fecha aprobado: 4 marzo 2009

