
¿ Introduction
The solitary plasmacytoma usually affects the bone tissue, but its extramedullary form, with incidence around 5%, may be related to secondary invasion by multiple myeloma.1 The primary form is extremely rare. We report the first case in the literature of pancreatic plasmacytoma diagnosed by ultrasound-guided fine needle aspiration (EUS- FNA).
¿ Case report
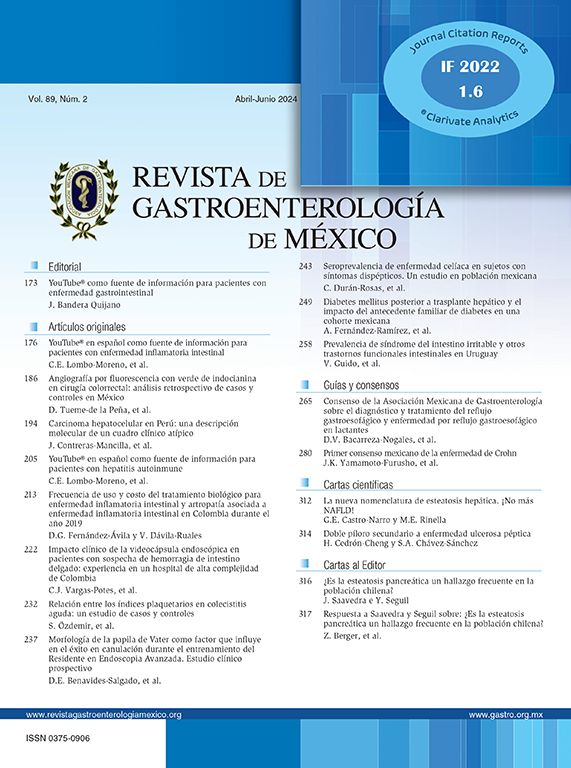
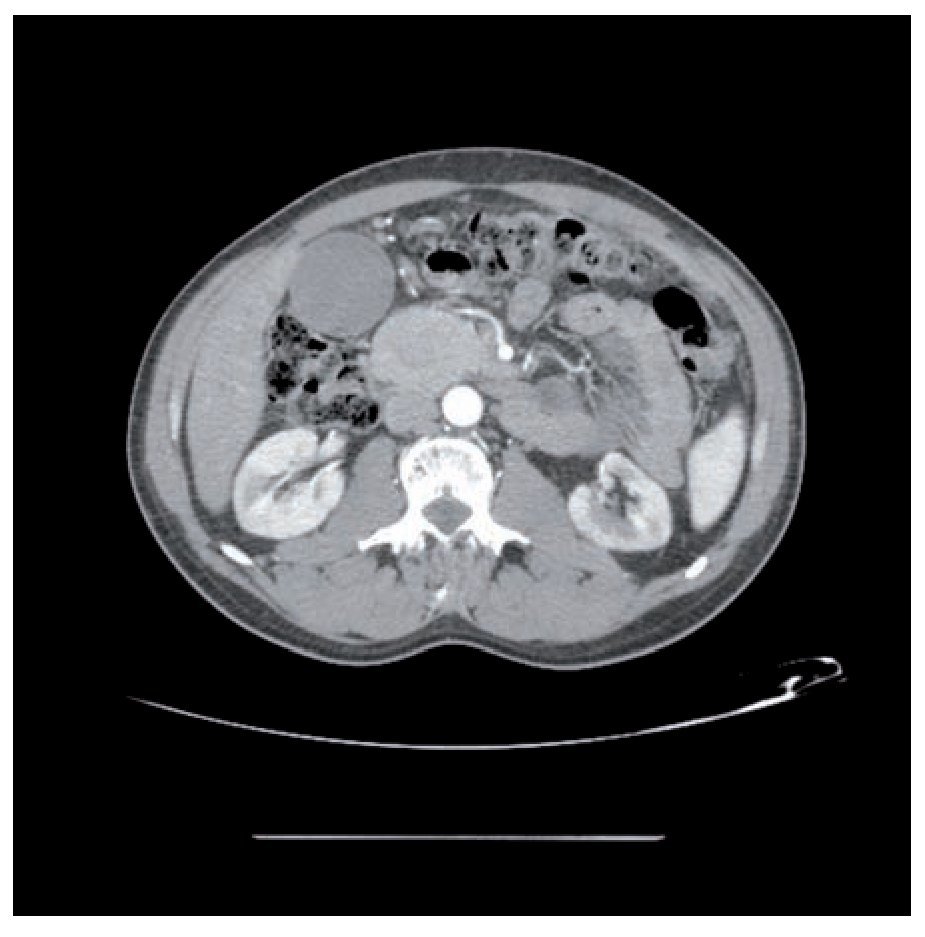
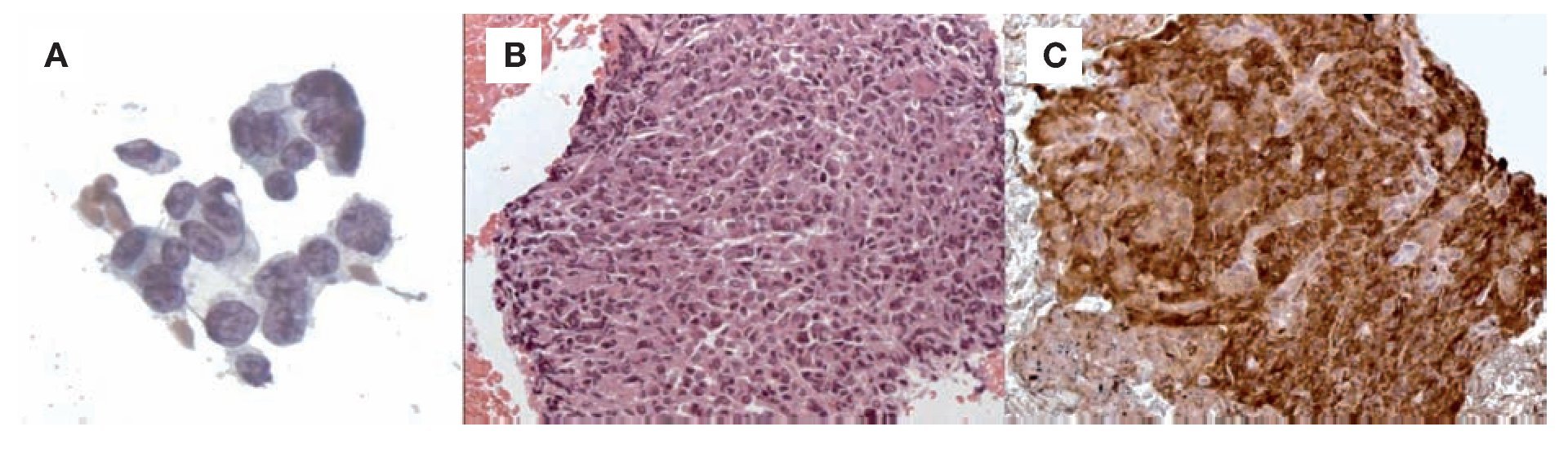
Forty-two years-old male patient, with diagnosis of solitary plasmacytoma in the right shoulder since 2002, was treated initially with local radio-therapy with resolution of the lesion. In December 2004, new plasmacytomas in knee and ankle were diagnosed and were treated with radiotherapy and steroids (dexamethasone). Good response was achieved, but in November 2007 a new plasmacytoma in the right thigh was diagnosed, and lambda light chain was detected in the urine. At this time, there were no target organ injuries or bone marrow plasmacytosis, but because of the multiple plasmacytomas systemic treatment was chosen. This treatment was conducted with radiotherapy and chemotherapy (cyclophosphamide, dexamethasone, thalidomide - seven cycles), without response. A new chemotherapy protocol with bortezomib, dexamethasone and thalidomide was started. After completing the second chemotherapy cycle of this protocol, the patient developed cholestatic jaundice and was admitted for investigation. A CT scan of the abdomen showed a large expansive lesion in the head of the pancreas (Figure 1). Patient underwent ERCP to clear the biliary tree and EUS was performed. This study showed hypoechoic and heterogeneous mass in the head of the pancreas. FNA was performed and samples were obtained for pathologic analysis (Figure 2). The cytology report revealed small cell neoplasm with immunohistochemical profile consistent with plasmacytoma producing lambda light chain (Figure 3).
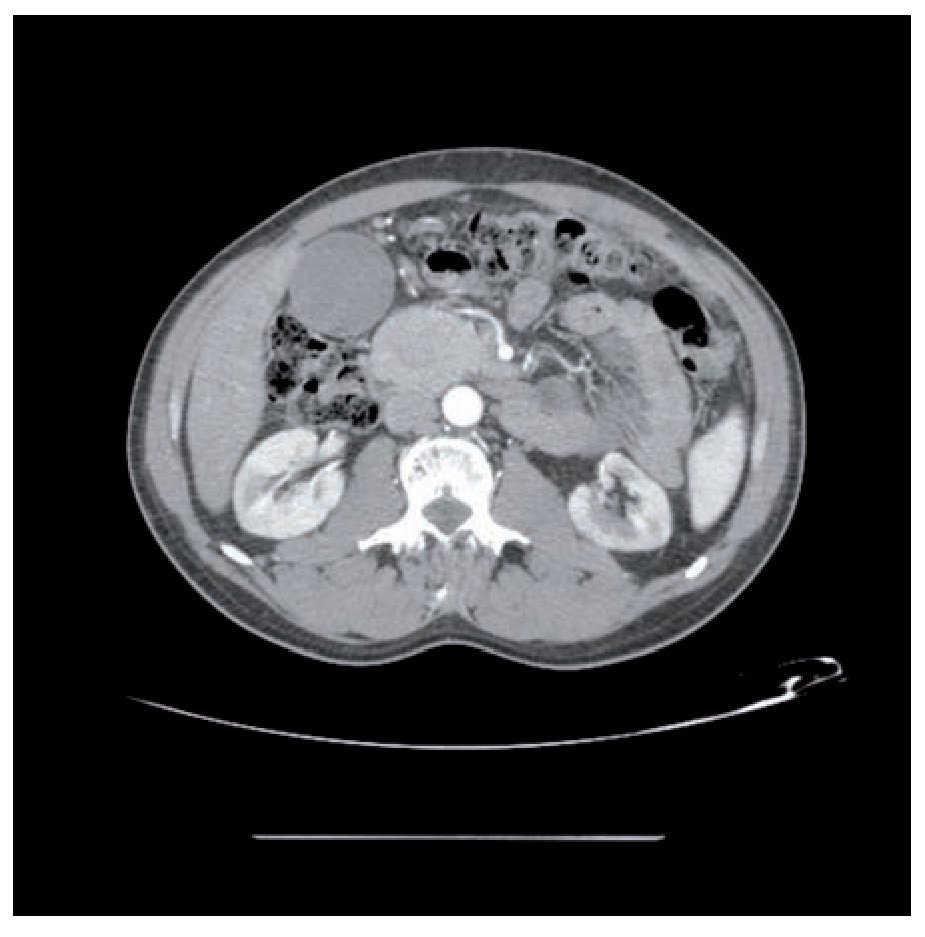
¿ Figure 1. CT scan showing a large and expansive lesion in the head of the pancreas.

¿ Figure 2. EUS showing hypoechoic and heterogeneus mass in the head of the pancreas.
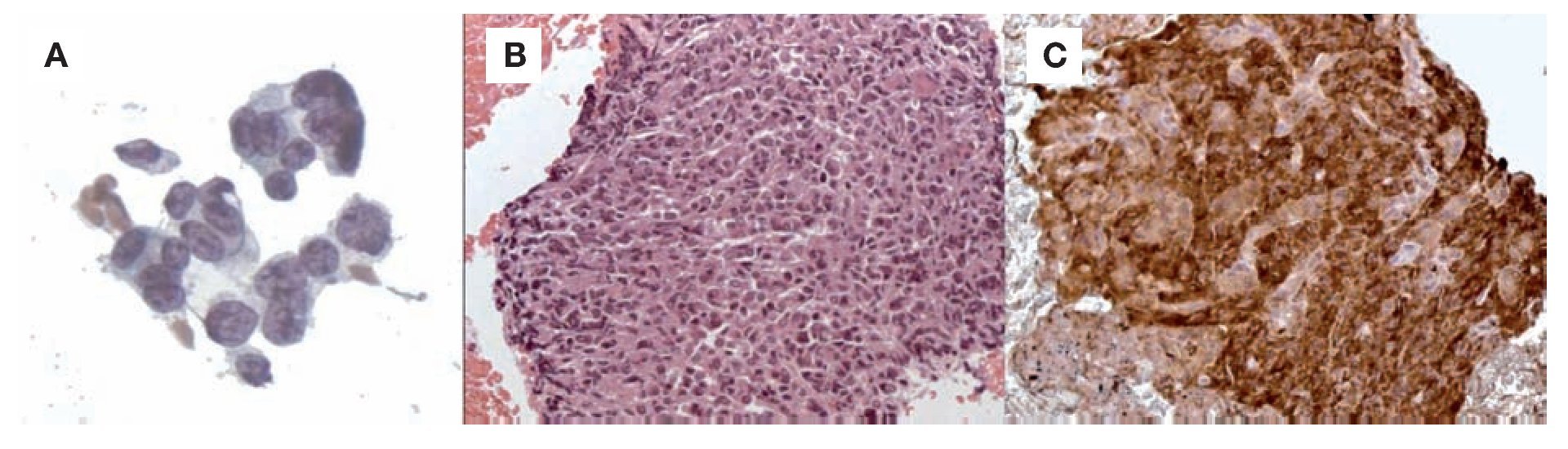
¿ Figure 3. A) cytology (1000x); B) H & E Staining - Paraffin (400x); C) lambda light chain (400x). All sequence of images confirmed the presence of plasma-cytoma.
Chemotherapy protocol was changed to bortezomib, dexamethasone and cyclophosphamide. Four cycles of chemotherapy were administered with partial response. Patient died because infectious complications after the fourth cycle f chemotherapy.
¿ Discussion
Extramedullary plasmacytomas are malignant tumors of monoclonal plasma cells. Progression to multiple myeloma is seen in approximately 11 to 30% of cases within 10 years. The group with highest incidence is composed of middle age men with aerodigestive tract involvement, especially in the head and the neck.1 The gastrointestinal tract involvement is uncommon, but the organ most commonly involved is the stomach.2 Rarely, the pancreas is infiltrated by plasmacytes, either as solitary plasmacytoma or extramedullary invasion by multiple myeloma.3-5 The diagnosis is based on the finding of extramedullary monoclonal plasma cells without proliferation of plasmacytes in bone marrow.6
Computed tomography (CT) is the most widely used method for assessing these cases. The most frequent location is the head, but there are reports of diffuse involvement 7 and two plasmacytomas in the same pancreas.8
The CT-guided fine needle aspiration can make the diagnosis.9 Due to the similar cytomorphology of the plasmacytes in relation to neuroendocrine cells, pancreatic extramedullary plasmacytoma can be mistakenly diagnosed as a neuroendocrine tumor. Immunohistochemistry for light chains, associated with neuroendocrine markers, is essential for the differential diagnosis,10 and it was demonstrated in the present case.
EUS showed a hypoechoic, heterogeneous, well defined mass in relation to the normal pancreatic echotexture, easily accessible to puncture, with the well known advantages over CT-guided puncture. This is the first case described in the literature of successful EUS FNA in the diagnosis of plasmacytoma.
Treatment options include surgery, radiotherapy, chemotherapy, and combinations of them.11 Studies indicate that this tumor is highly radiosensitive and chemosensitive.2,12,13 However, as in our case and in other studies,11,14 the prognosis and the chemotherapy sensitivity can be poor and the disease course can be very aggressive.
Correspondence: Everson L. A. Artifon, M.D., Ph.D, F.A.S.G.E. Director, Biliary and Interventional Endoscopy - Ana Costa Hospital; Associate
Professor of Medicine-University of Sao Paulo. Rua Guimaraes Passos, 260 - Apto 121, Vila Mariana, Sao Paulo-SP, Brazil, 01508-010
Phone / Fax: 55-11-3069-6221.
Email: eartifon@hotmail.com
Recibido el 13 de abril de 2010;
aceptado el 23 de abril de 2010.

