¿ Introduction
Heartburn is a very common symptom;1 40% of the general population is estimated to present an episode each month, and at least 20% present an episode each week.2,3 It is defined as a hot or burning sensation that begins in the epigastrium or thorax and radiates into the throat.4 It is the cardinal symptom of gastroesophageal reflux disease (GERD).5 The symptoms induced by GERD are considered the principal cause of office visits to the gastroenterologist and represent a significant cost to healthcare systems.6 GERD has three different phenotypic presentations:7,8 none-rosive reflux disease (NERD), erosive esophagitis (EE), and Barrett's esophagus (EB).
The pathophysiology of heartburn is complex. The stimulation of chemoreceptors by acid reflux is considered the principal etiologic mechanism. There is evidence, however, that points to other causes, such as gastroduodenal reflux,10-12 an alteration in esophageal contractility,13,14 and esophageal hypersensitivity15-17. The latter has been defined as abnormal nociception. There are different esophageal patterns of chemosensitivity and mechanosensitivity in the various phenotypes of GERD.18 The sensitivity to acid or chemosensitivity is evaluated by the Bernstein test and those with an abnormal exposure to acid are the most chemosensitive.19
The presence of type 1 vanilloid receptors (VR1), currently called TRPV1 (transient receptor potential vanilloid-1), has been recently described on C-type sensory (afferent) neurons of the gastrointestinal mucosa.20-23 The activation of TRPV1 occurs as a result of heat, acid, lipoxygenase products, anandamine, and its well known agonist capsaicin. TRPV1 activation sets in motion a cascade of important physiologic events, such as the release neurotransmitters, including substance P and calcitonin gene-related peptide.24,25 Some authors have suggested that heartburn is mediated by TRPV1 receptor stimulation.26,27 Recently, the intraesophageal instillation of capsaicin in healthy volunteers was shown to produce heartburn, chest pain and burning, and epigastric pain.27,28 Capsaicin is the pungent component of chilli and currently the most studied TRPV1 receptor agonist.29,30
The aim of the current study was to investigate the effect of intraesophageal instillation of capsaicin on the induction of esophageal symptoms, as well as its role in esophageal chemo-sensitization to acid in the different GERD phenotypes.
¿ Methods
Patient Selection: Patients older than 18 years of age consecutively diagnosed with GERD - defined as experiencing heartburn or acid regurgitation at least two times a week31 - and healthy volunteers were prospectively included. GERD patients were classified into three groups: 1) NERD, patients who had an abnormal 24-hour esophageal pH monitoring -% total pH below 4 > 4.2%32,33 - and a negative endoscopy; 2) EE, patients with mucosal erosions of the esophagus according to the Los Angeles classification;4,35 and, 3) Barrett's esophagus, patients with specialized intestinal metaplasia.36,37 Exclusion criteria were pregnancy or lactation, ingestion of proton bomb inhibitors seven days before the study, use of drugs that modify visceral sensitivity (e.g., antidepressants), uncontrolled comorbidity such as diabetes mellitus, hypertension, hypothyroidism, connective tissue disease, or history of gastrointestinal surgery except cholecystectomy or appendectomy. Patients were also excluded if esophageal intubation was not possible through a nasal approach.
The Instituto Nacional de Ciencias Médicas y Nutrición Institutional Ethics and Investigation Review Board approved the protocol for this study and all participants signed an informed consent form.
Demographic data and GERD symptom duration were registered. The Carlsson-Dent questionnaire (CDQ), which explores the presence of GERD related symptoms, was applied to all participants and was considered positive if >4.38
Esophageal sensitivity to capsaicin:
a) Capsaicin and acid perfusion. A manometric catheter (diameter = 4.5 mm, Zinetics, Medtronic) was placed in the middle third of the esophagus through a nasal approach. Participants were randomized to receive esophageal perfusion with either saline solution (control) or capsaicin. Thirty minutes later all participants received an intraesophageal infusion of 0.1N hydrochloric acid. A week later those who had received saline solution received capsaicin perfusion and vice versa. After a 2-minute stabilization time, the esophagus was perfused with 3 mL of 0.9% saline in one minute or 3 mL of a 0.17 mg/mL capsaicin solution (Sigma Aldrich, Vienna, Austria). Esophageal and gastric symptoms were evaluated every five minutes for half an hour. Thereafter, 0.1 N hydrochloric acid was perfused at a rate of 6 mL/min for 10 minutes with an infusion pump.28 Symptom severity was registered during hydrochloric acid perfusion and afterwards every 5 minutes for 20 minutes.
b) Symptom evaluation. Five symptoms were investigated in order to evaluate esophageal sensitivity: 1) chest burning, a burning sensation in the medial region of the anterior thorax; 2) chest pain, an oppressive sensation in the medial region of the anterior thorax; 3) heartburn, a burning sensation that begins in the epigastrium or thorax and radiates into the throat; 4) epigastric burning, a burning sensation in the epigastrium; and, 5) epigastric pain, non-burning epigastric pain. Symptom duration was registered. A 20 cm visual analog scale (VAS) was used to evaluate symptom severity. This scale incorporated descriptions on the left-hand side, including: no sensation, minimal sensation, very weak, weak, very slight, slight, moderate, barely strong, slightly strong, strong, intense, very intense, and extremely intense.39
Statistical analysis: Qualitative variables were described in terms of absolute and relative frequencies, while quantitative variables were described as mean and standard deviation. The area under de curve (AUC) was calculated for the severity of each symptom during the 30 min experiment. A total esophageal symptom score was calculated by adding the AUC for severity of each symptom (pain, chest burning, and heartburn) in every participant. The Kruskal-Wallis test was employed for comparisons between groups. The Wilcoxon test was used to analyze differences between saline and capsaicin perfusion and between the first and second acid perfusion. The c2 test was conducted to compare proportions. Statistical significance was set at a p < 0.05.
¿ Results
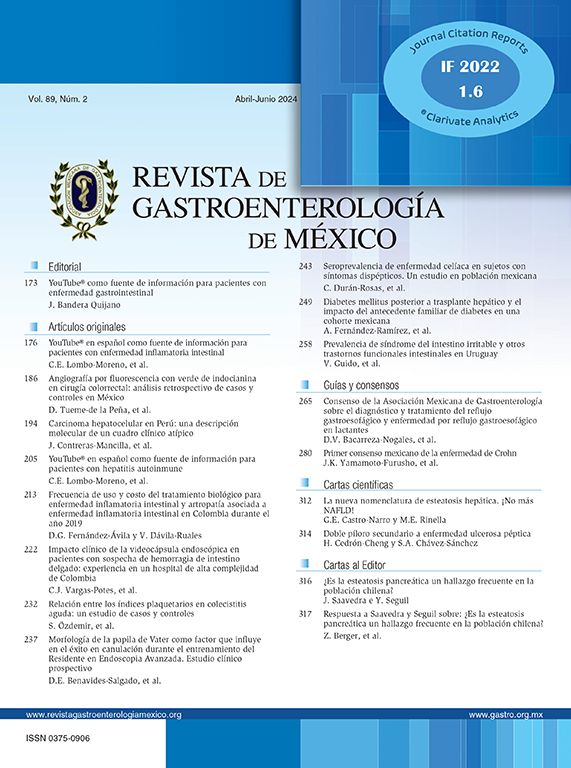
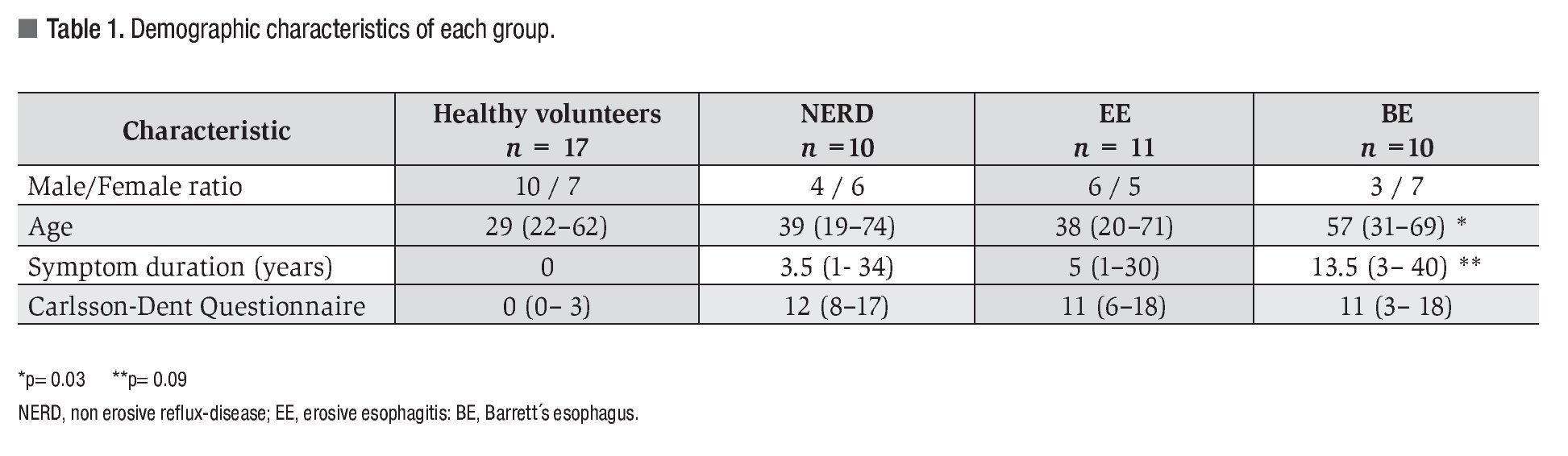
Forty-eight participants were included, 25 of them women (52%), with a mean age of 41 years (range 19-74 years). Of these participants 17 were healthy volunteers, 10 patients had NERD, 11 had EE, and 10 had BE. Demographic data, GERD duration, and CDQ score are shown in Table 1. Patients with BE had a greater proportion of male gender, higher mean age, and longer GERD duration.
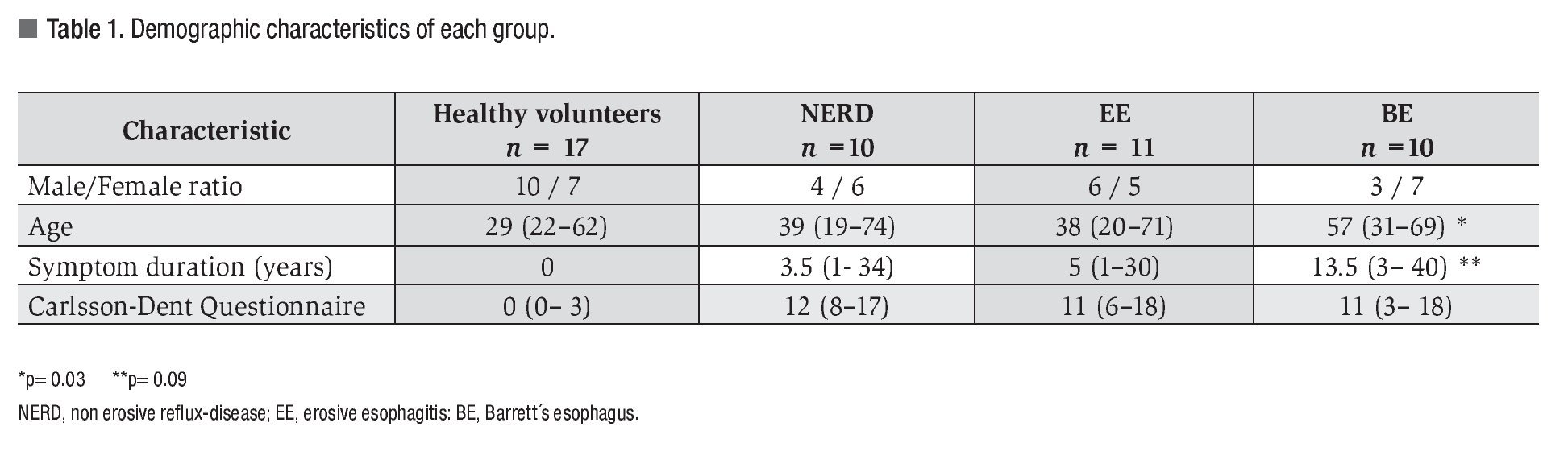
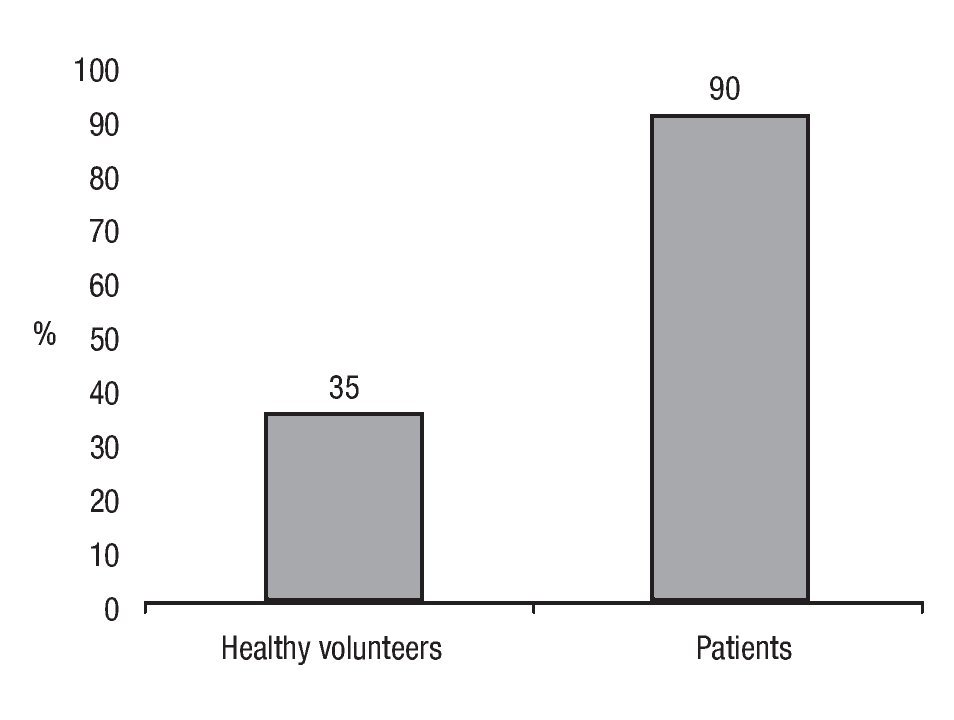
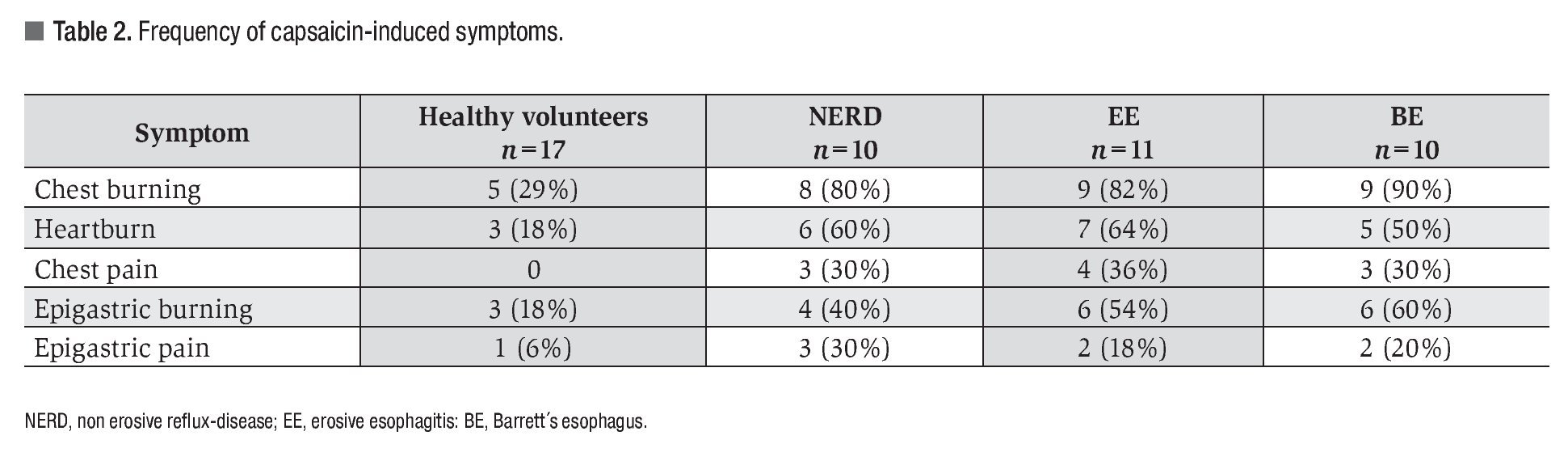
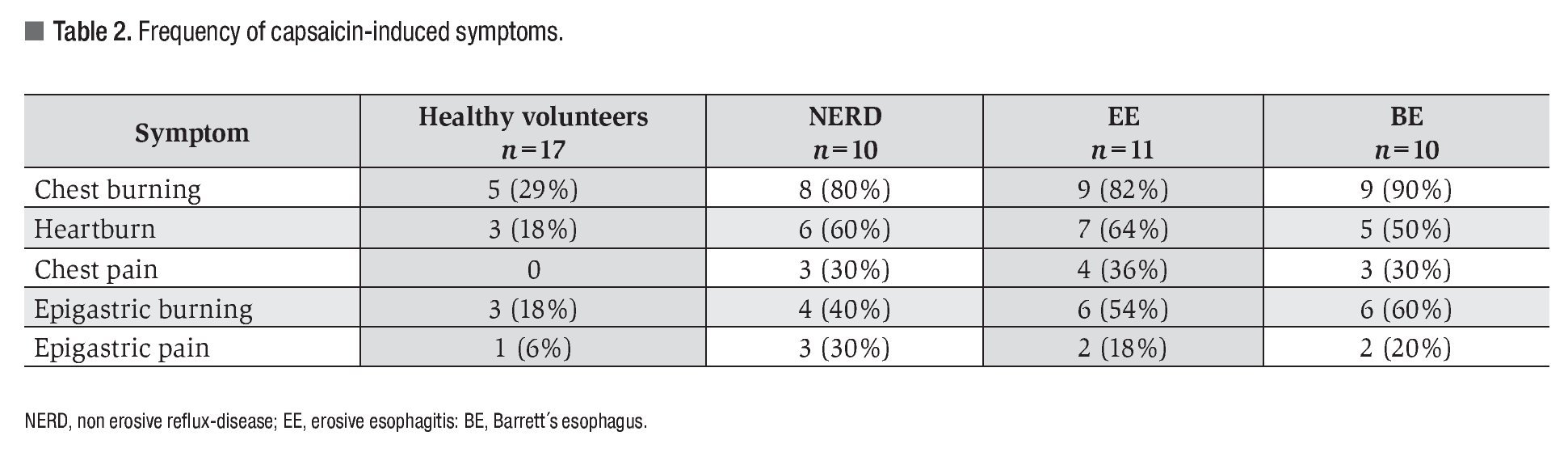
Capsaicin-induced symptoms: After capsaicin perfusion 28 of the 31 patients (90%) and 6 of the 17 (35%) healthy volunteers presented esophageal symptoms (Figure 1). Chest burning was the most frequent capsaicin-induced symptom. Of the 48 patients 31 (65%) presented chest burning, 21 (44%) presented heartburn, and 10 (21%) presented chest pain (Figure 2). No difference in frequency of the different capsaicin-induced symptoms was found among the GERD subgroups. Of the 48 participants 19 (40%) and 8 (16%) reported epigastric burning and pain, respectively (Figure 2). Esophageal and gastric symptom distribution in each of the GERD subgroups is presented in Table 2.
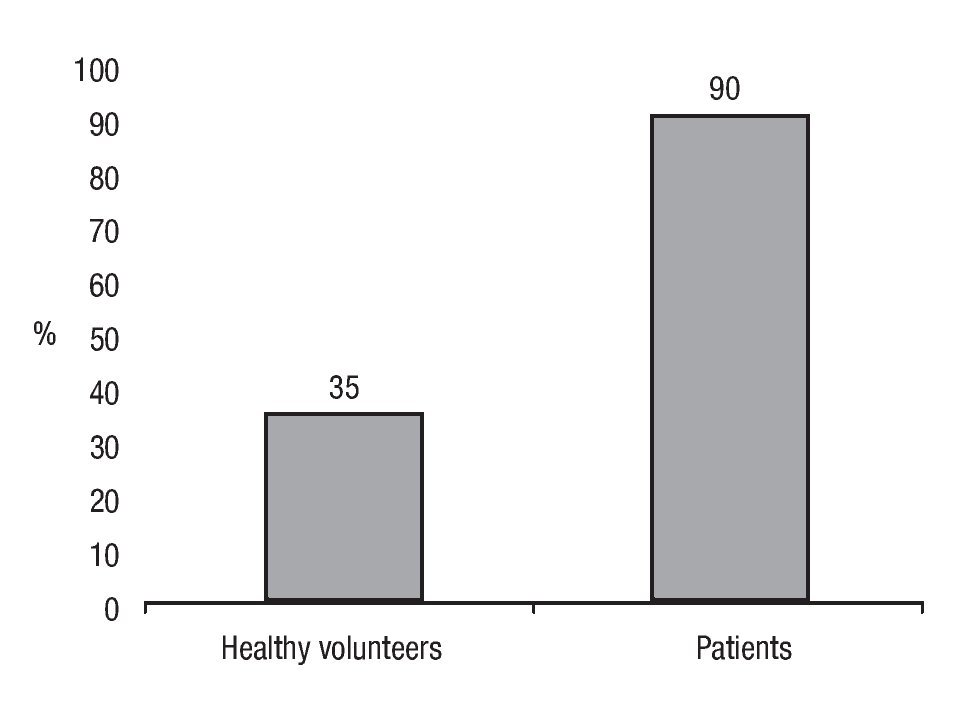
¿ Figure 1. Esophageal symptom frequency after capsaicin infusion.
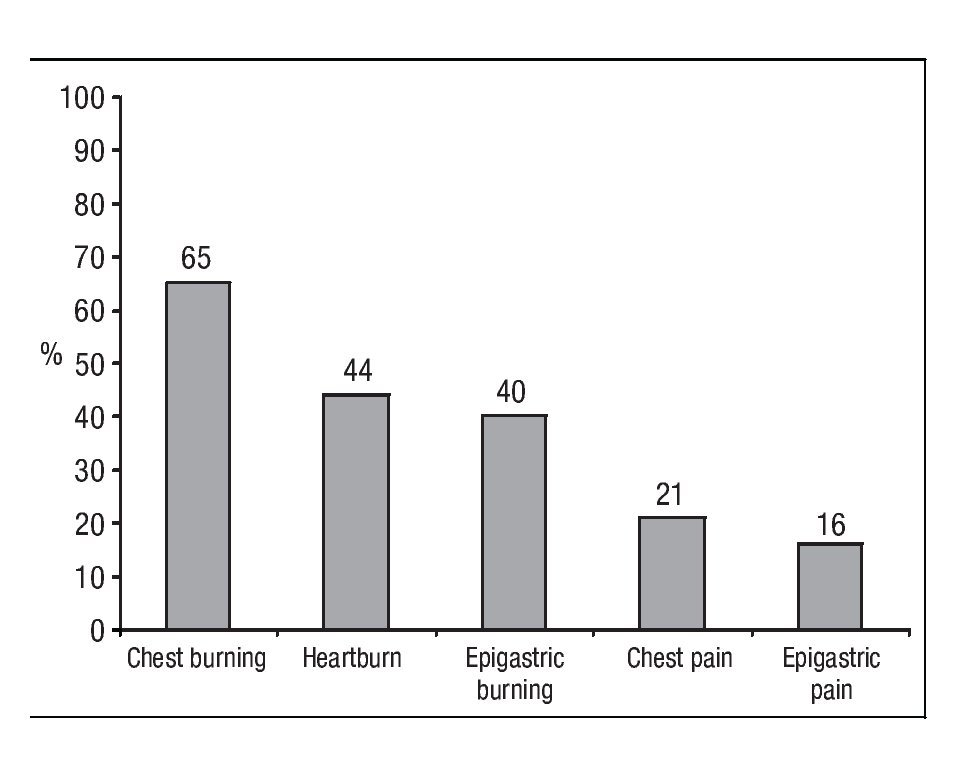
¿ Figure 2. Frequency of symptoms induced after capsaicin perfusion.
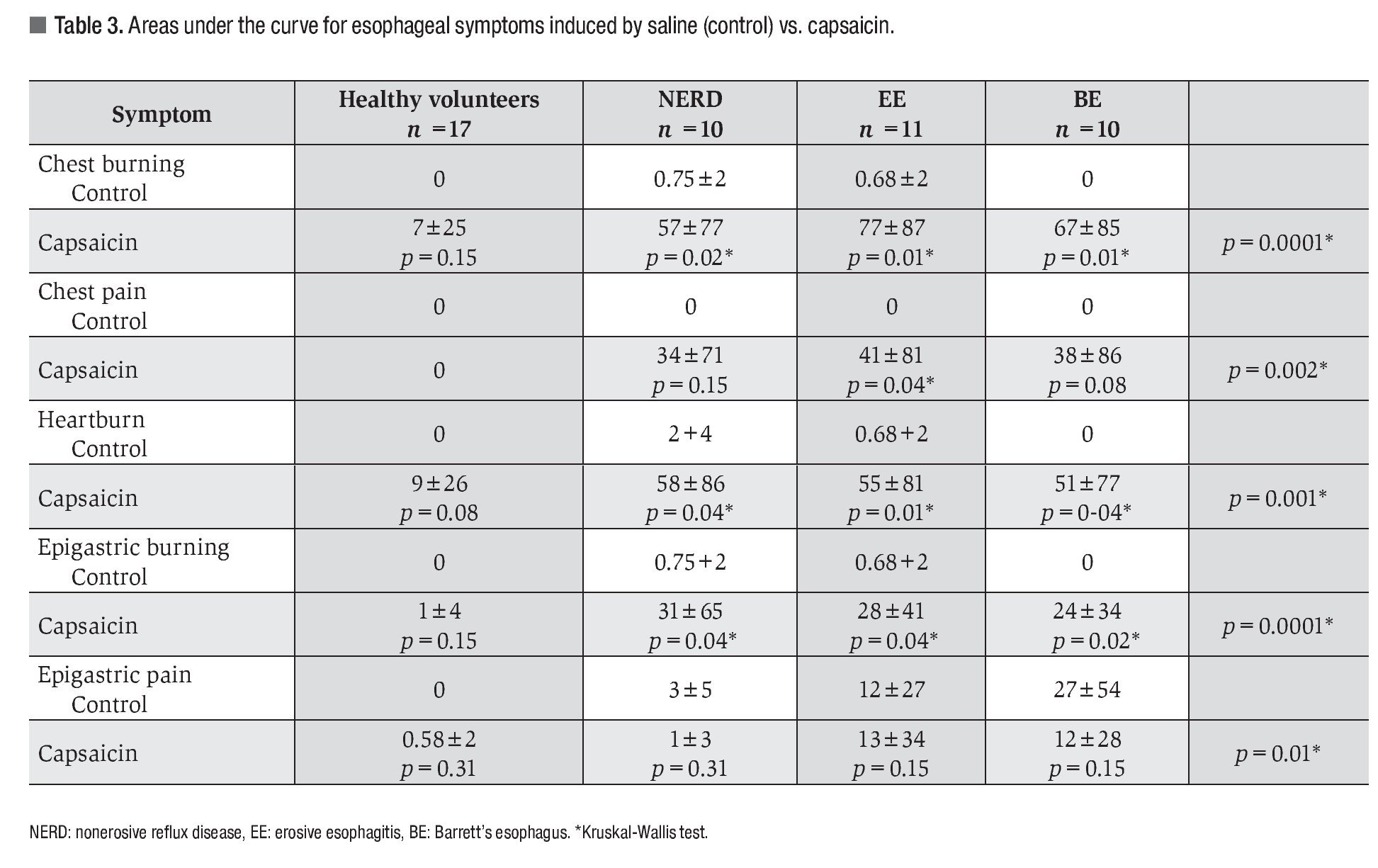
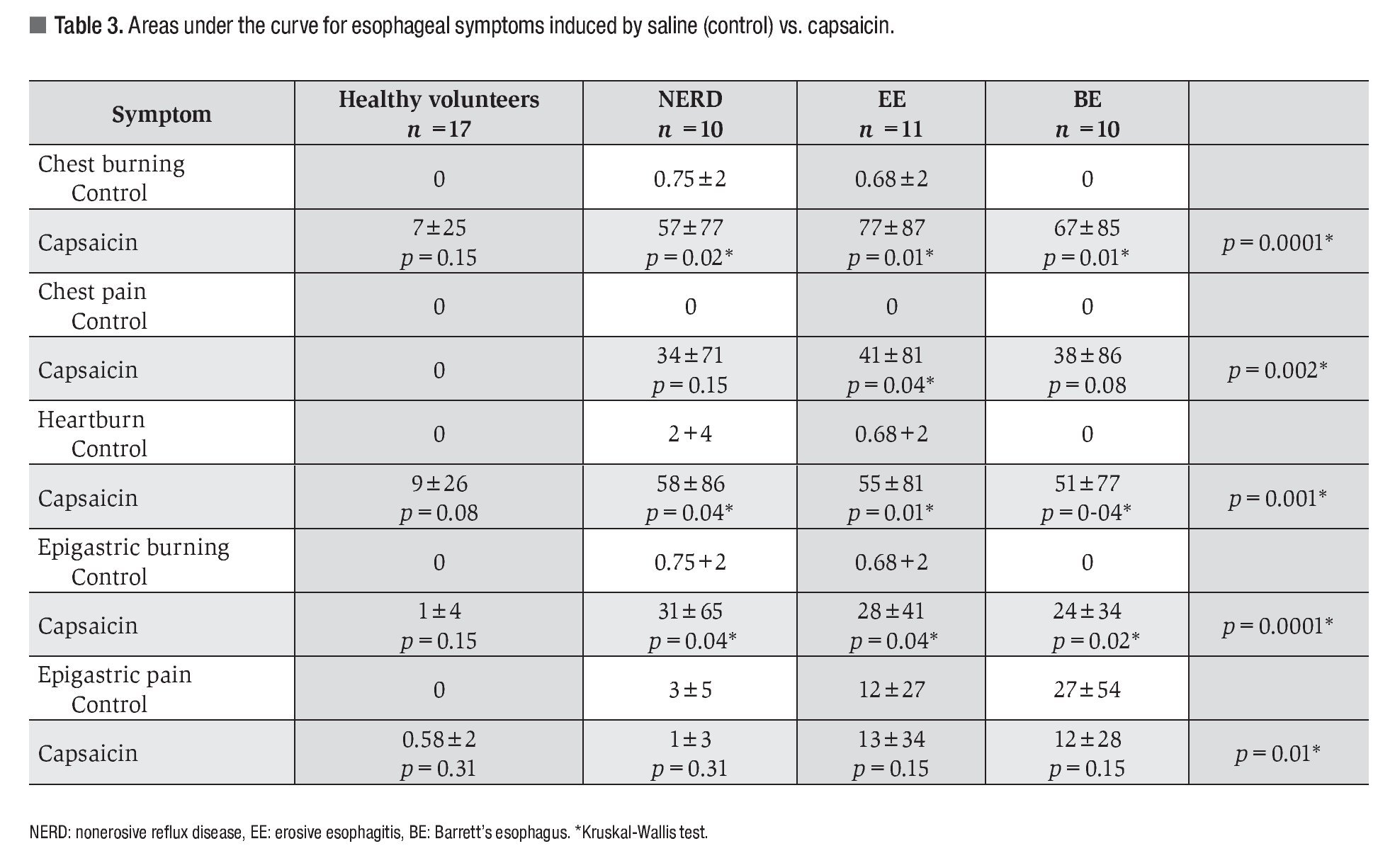
AUC for esophageal and gastric symptom severity after saline or capsaicin infusion are shown in Table 3. No significant differences in the AUC for esophageal and gastric symptoms were observed after saline or capsaicin infusion in healthy volunteers. Mean AUC for the 5 capsaicin-induced symptoms was significantly greater in patients with GERD. The greatest symptom severity was seen in patients with EE, although this difference was not significant. With respect to gastric symptoms, only the AUC for epigastric burning was significantly greater in patients with GERD compared to healthy volunteers.
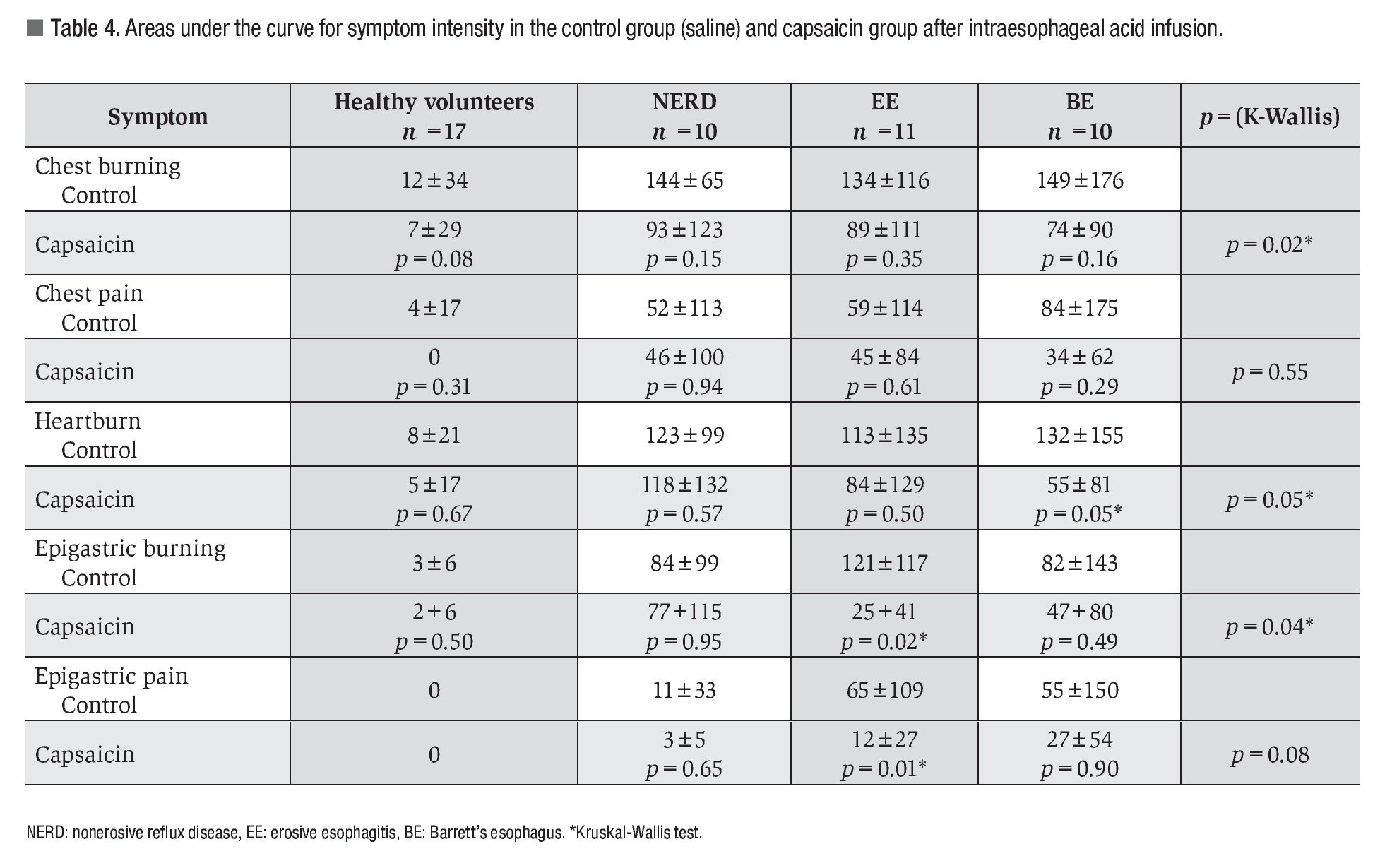
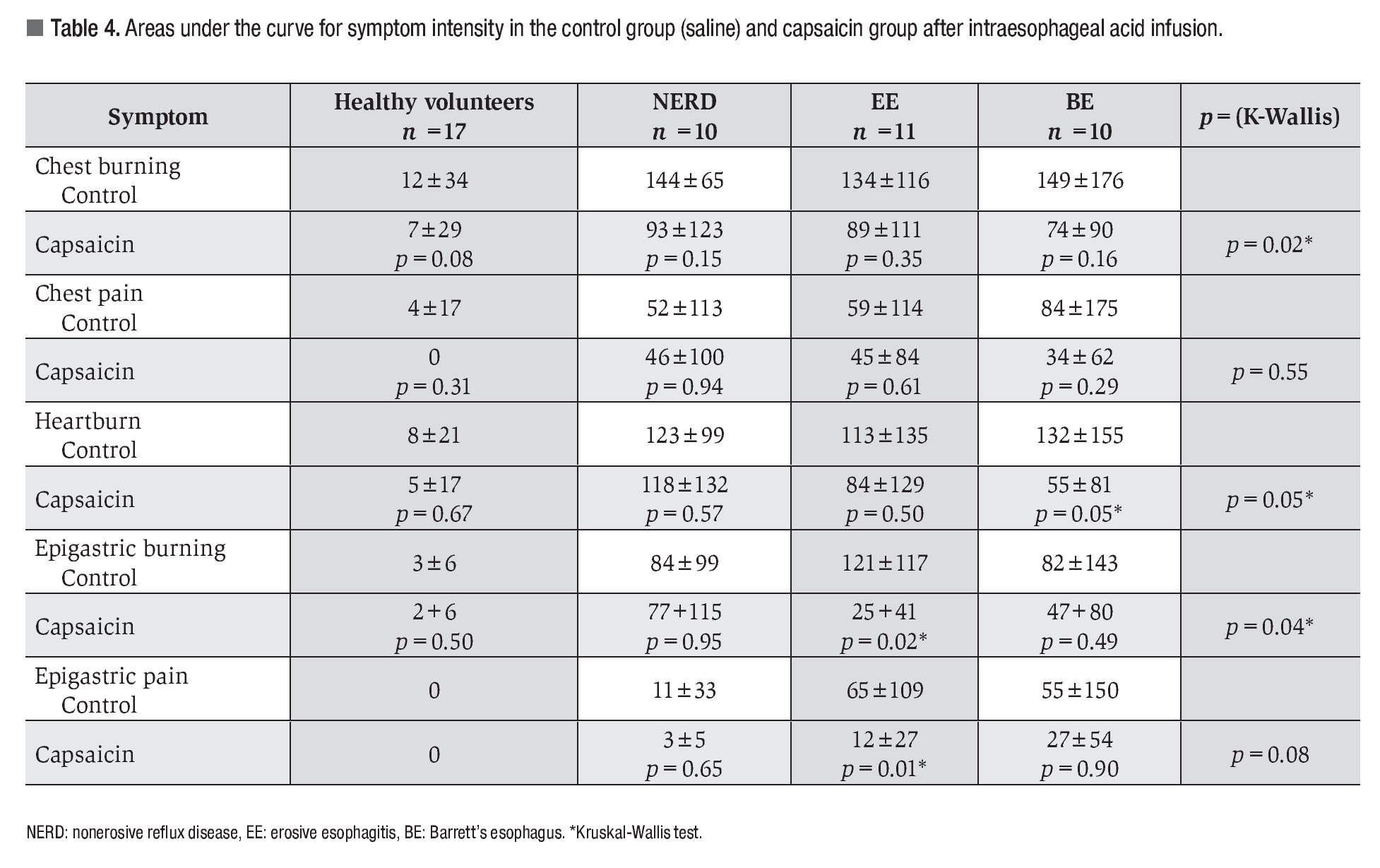
Esophageal and gastric chemosensitivity to acid: The AUC for esophageal and gastric symptoms after acid perfusion in both controls and patients with capsaicin infusion are shown in Table 4. Capsaicin perfusion decreased the AUC for all 5 evaluated symptoms in both healthy volunteers and GERD patients. It also significantly decreased the severity of chest burning, epigastric burning, and heartburn after acid infusion in GERD patients compared to healthy volunteers. In the BE subgroup heartburn was significantly less after capsaicin administration. Epigastric burning and pain caused by acid perfusion were significantly decreased in patients with EE after capsaicin infusion.
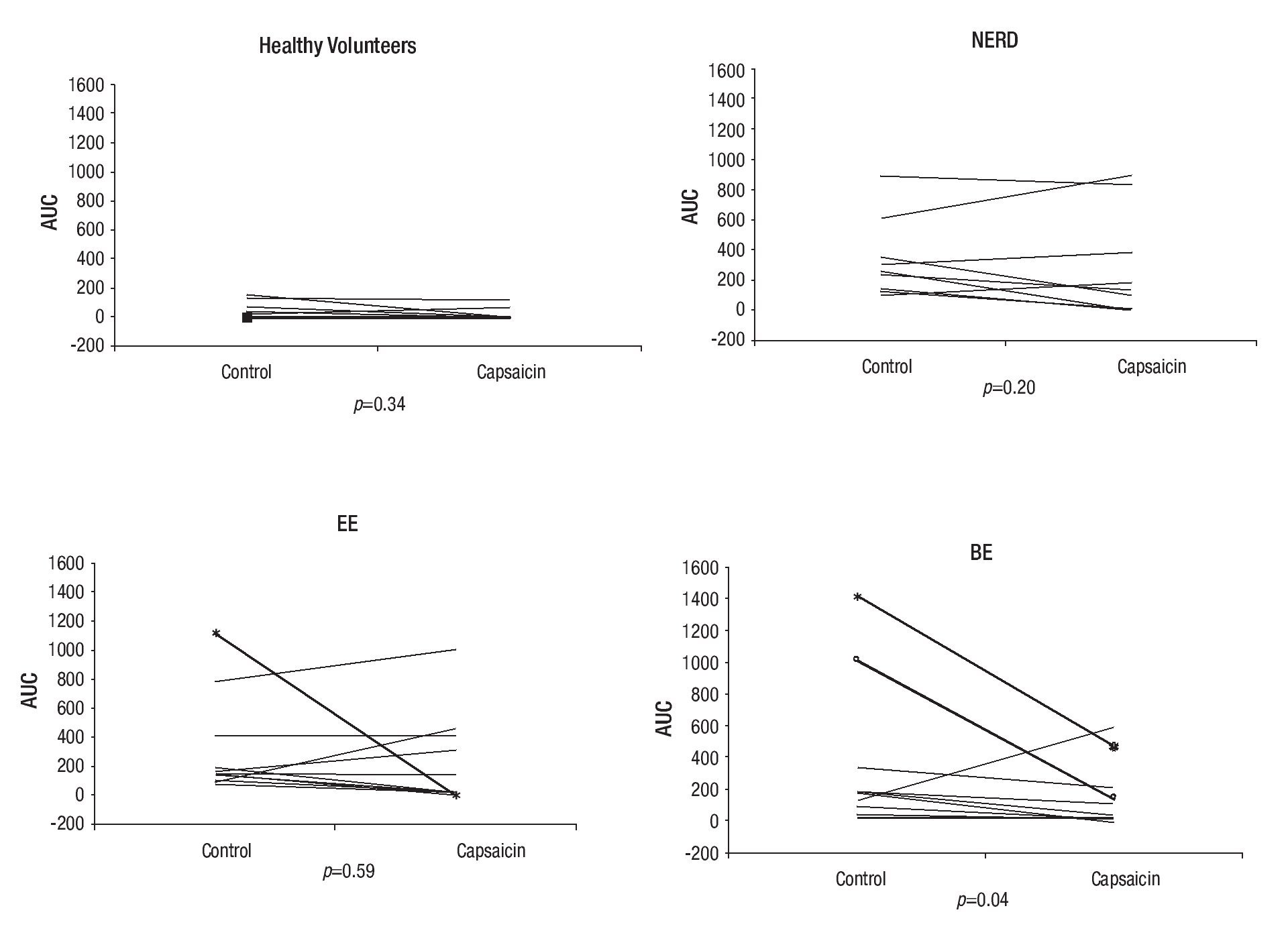
The total esophageal symptom severity score during acid perfusion decreased significantly after capsaicin administration in patients from the BE subgroup (Figure 3).
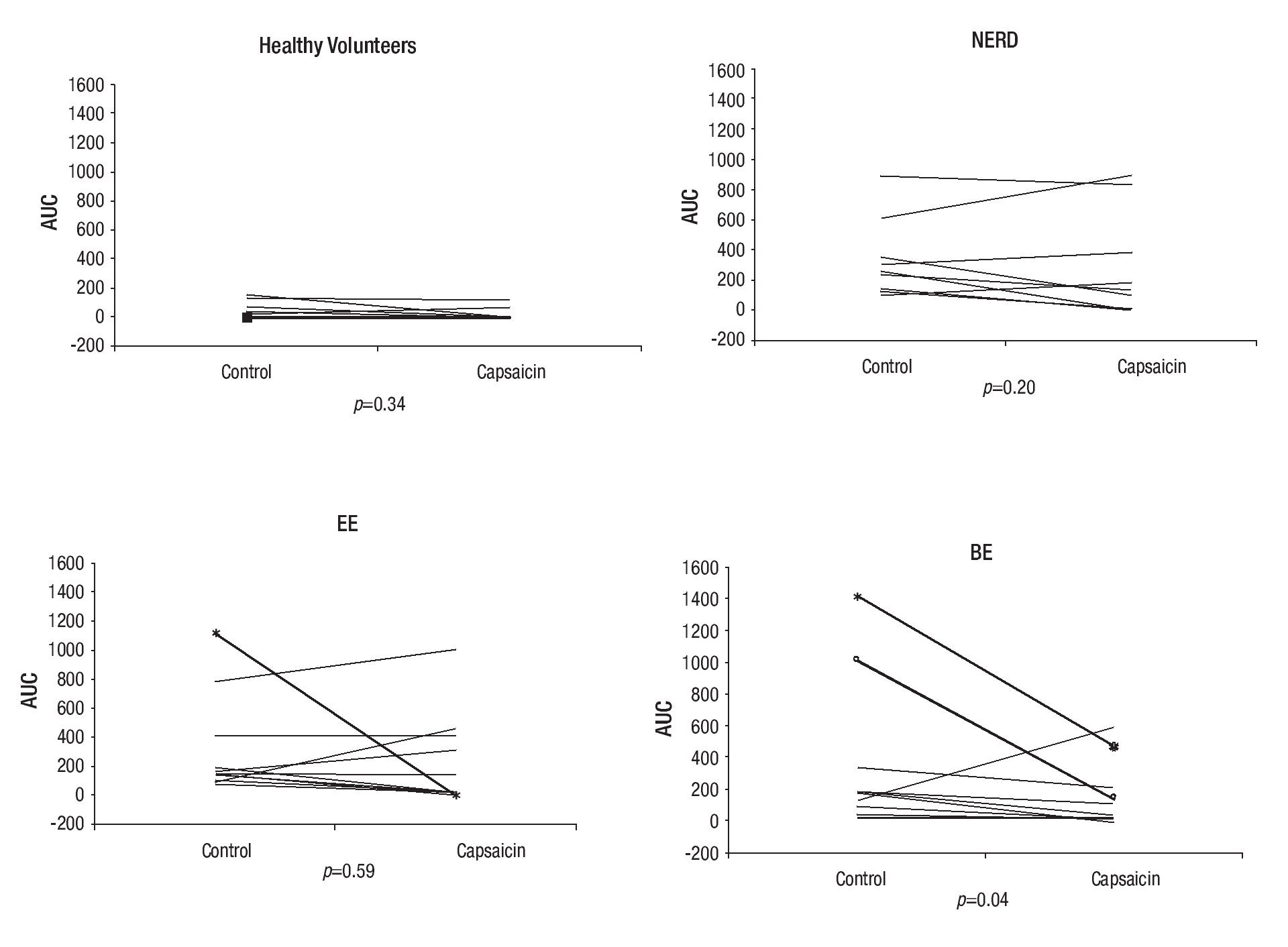
¿ Figure 3. Composite score of AUC for esophageal symptom intensity in the control group (saline) and capsaicin group after intraesophageal infusion of acid.
Acid perfusion was interrupted due to esophageal and gastric symptoms graded as extremely intense in three female patients, two of them with BE and one with EE. After capsaicin administration, however, these three patients completed and tolerated acid infusion (Figure 3).
¿ Discussion
Capsaicin (8-methyl-N-vanillyl-6-nonenamide) is the pungent ingredient of chilli and has been used in diet and in medicinal remedies for hundreds of years. It was synthesized in 1923 and its homovanillic moiety is essential for its biologic activity.40 Capsaicin has been proven to have various pharmacologic effects; among the most studied is its capacity to decrease the nociceptive sensitivity of different organs. Currently, capsaicin is used in the management of detrusor hyperreflexia,41 vasomotor rhinitis,42 pruritus in psoriasis and uremia,43 and as an adjuvant analgesic in neuropathic pain like postherpetic neuralgia,44 diabetic neuropathy45 and postmastectomy pain syndrome.46 It has been also been used as a topical analgesic. Recently, capsaicin has been investigated in the management of esophageal motility disorders,47,48 functional dyspepsia,49 and rectal incontinence.22
Capsaicin stimulates the type 1 vanilloid receptor (VR1), also called TRPV1 (transient receptor potential vanilloid type 1). TRPV1 is a nonselective cationic channel that is predominantly expressed on type C unmyelinated small caliber sensory neurons. TRPV1 can also be found in nonneuronal tissue as well as in the gastrointestinal mucosa. TRPV1 stimulation releases various neurotransmitters, namely substance P (SP) and the calcitonin gene-related peptide, both of which are pain mediators. TRPV1 acts as a molecular integrator of physical and chemical stimuli at nociceptive nerve endings.50
There is evidence that TRPV1 is present in the gastrointestinal mucosa. Domotor et al,21 found that vanilloid receptor distribution varies according to disease entity, such as gastritis, ulcer disease, colonic polyps, intestinal inflammatory disease, and adenocarcinoma of the colon.
Various studies have shown the presence of TRPV1 in the esophagus and have found a possible association between TRPV1 and esophageal symptoms. Bhat et al,51 determined the expression of TRPV1 in 39 patients with NERD. Patients with increased acid exposure have increased expression of TRPV1. This suggests that pathologic exposure to acid is associated to changes in esophageal innervation with increased expression of TRPV1 in the absence of macroscopic lesions. Matthews et al,26 showed a higher percentage of TRPV1 in 7 patients with EE compared to controls. In a comparative study in patients with different GERD phenotypes, Dickman et al,52 proved that patients with non-erosive reflux disease had increased expression of TRPV1 in the proximal esophagus as compared to the other GERD phenotypes.
TRPV1 receptor stimulation with capsaicin induces esophageal symptoms. In healthy subjects, Rodriguez et al,53 showed that the ingestion of a high-fat diet that included capsaicin produced heartburn of higher severity than high-fat diet without capsaicin. Bhalla et al,27 also showed that intraesophageal injection of capsaicin produced heartburn and chest pain. On the other hand, Kindt et al,28 instilled low-dose and high-dose caps-aicin in the esophagus of 10 healthy volunteers. They found that esophageal symptoms were dose dependent and that the most frequent symptom was chest burning. These authors suggested that stimulation of TRPV1 could be responsible for heartburn in GERD patients.
The current study evaluated esophageal and gastric symptoms induced by acute capsaicin administration in different GERD phenotypes. In this study, esophageal capsaicin perfusion produced diverse esophageal symptoms of varied severity in both healthy volunteers and GERD patients. Our study showed that capsaicin perfusion in GERD patients produced significantly higher symptom frequency and severity than the same perfusion in healthy volunteers. As was shown in the study by Kindt et al,28 the most frequent esophageal symptoms after capsaicin infusion were chest burning and heartburn. These findings support a possible association of esophageal inflammation and exposure to acid to the degree of TRPV1 expression. This study, however, was unable to detect a difference among different GERD phenotypes, perhaps because of the small sample size of each group.
There is evidence that exposure of TRPV1 to capsaicin causes activation of the receptor with subsequent desensitization. The desensitization caused by capsaicin appears to be different in acute versus chronic exposure. Kindt et al,28 performed an acid perfusion test after intraesophageal administration of high-dose and low-dose capsaicin in healthy volunteers. They too did not find a significant decrease in esophageal chemosensitivity after capsaicin administration. This suggests that a different receptor is responsible for esophageal sensitivity to acid. In the present study capsaicin did not decrease chemosensitivity to acid in healthy volunteers. However, administration of intraesophageal capsaicin did significantly decrease the AUC for severity of esophageal and gastric symptoms during and after acid perfusion. This further supports the concept that TRPV1 can be desensitized to acid stimulus with capsaicin, at least in conditions with increased inflammation or esophageal exposure to acid.
Exposure of the esophageal mucosa to capsaicin in patients with heartburn produced an analgesic effect after an initial phase of symptomatic worsening in one study.53 In another study, repetitive administration of capsaicin-containing chili powder in dyspeptic patients produced symptomatic improvement.49 These two studies demonstrate the desensitizing effect of repeated doses of capsaicin in both esophageal and gastric mucosa; and suggest TRPV1 as a possible therapeutic target in patients with heartburn or dyspepsia.
In conclusion, capsaicin induces esophageal and gastric symptoms in both healthy volunteers and GERD patients. The most frequent symptom associated to capsaicin infusion is chest burning. Capsaicin decreases esophageal chemosensitivity to acid in patients with GERD. These results imply that capsaicin might have a therapeutic utility, to decrease esophageal sensitivity to acid in GERD patients.
More prospective studies are required to evaluate the effect of repeated and chronic capsaicin administration in GERD patients.
Correspondence: Dr. Miguel Ángel Valdovinos Díaz.
Head of the Gastrointestinal Motility Laboratory INCMNSZ. Vasco de Quiroga N° 15. Col. Sección XVI, Del. Tlalpan, México D.F., CP 14000.
Telephone: 55 5573 1200 ext. 2706.
E-mail: mavaldo@quetzal.innsz.mx.
Received June 26th, 2010;
accepted July 6th, 2010.

