

We present the case of a 65-year-old woman with chronic constipation for 10 years that did not improve through dietary or drug treatment, and so she underwent total colectomy with intracorporeal ileorectal anastomosis with transvaginal specimen extraction. The procedure is called Natural Orifice Specimen Extraction (NOSE) and is used in both benign and oncologic resections with excellent results. The case presented herein is the first surgery for treating colonic inertia utilizing this technique that has been performed in Panama.
Constipation affects 2 to 34% of the patient population of the Western world.1 Colonic inertia is a syndrome characterized by chronic constipation due to slow colon transit that is refractory to drug treatment. In these cases, metabolic, pharmacologic, and organic causes are ruled out first. Only 9.9% of the patients with constipation diagnosed with colonic inertia that is refractory to medical treatment are surgical candidates, as was the case with our patient. The studies carried out were: colonoscopy with no pathologic findings, colon transit time that reported colonic inertia, and defecogram and manometry whose results were within normal limits.
Total colectomy with ileorectal anastomosis is the best available therapeutic option. It is a complex procedure, but with the advent of laparoscopic surgery and its advantages in relation to the cosmetic effects, hospitalization, recovery, and complications,2 this type of procedure is being performed more often.
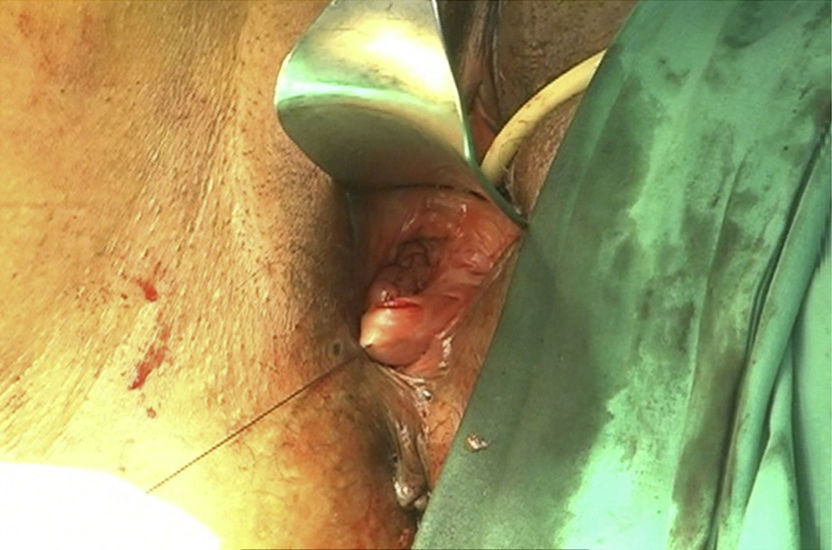
With prior liquid diet and colon cleansing, the patient was placed in the lithotomy position and given general anesthesia. A 10mm trocar was placed using the open Hasson technique and insufflation of the pneumoperitoneum was begun. A 10mm camera with a 30° lens was introduced, and the rest of the trocars were placed under direct vision at the right and left quadrants and at the epigastrium. The distal ileum was sectioned with Endo-GIATM and the colon was resected using the medial to lateral approach. The rectum was then sectioned with Endo-GIATM at the level of the promontorium. Posterior colpotomy with cautery was performed and the specimen was extracted transvaginally (Fig. 1). The vaginal defect was closed with absorbable monofilament suture (Fig. 2), an anvil was placed at the distal end of the ileum and attached with 2-0 monofilament. A circular transrectal EEA25 stapler was introduced and the ileorectal anastomosis was stapled, with a negative pneumatic test. The patient passed gas and began a diet 48h later. She was released with good progression on the third day and had normal postoperative controls. The patient's postoperative evaluations of the anorectal and vaginal physiology have been satisfactory.


Colonic inertia is currently treated with total colectomy and ileorectal anastomosis with good long-term results. In a study conducted by the Universidad Católica de Chile,2 20 laparoscopic total colectomies with ileorectal anastomosis were performed with similar results to those of the open technique, as well as better results in relation to recovery, the cosmetic aspect, and fecal continence, as well as no deaths.
There are 2 NOSE modalities for colorectal surgery: transanal and transvaginal. The first demands greater colon preparation and proctoscope use as confirmed by Knol et al.3 In a case series reported by Saad and Hosogi4 on patients with oncologic indications and diverticular disease, a McCartney tube was inserted for placing the anvil to be used in the colorectal anastomosis. The oncologic margin was adequate in the malignant cases, with no complications and with excellent results regarding postoperative pain. In the comparison of transanal and transvaginal extraction, the transanal approach has limitations when the diameter of the rectum is small, when there is rectal stricture, and when there is the probability of fecal contamination due to opening of the rectum, as well as the possibility of fecal incontinence from damage to the sphincters upon extracting the specimen.
In 2008, Franklin et al. reported the first case in the United States of a right hemicolectomy with transvaginal specimen extraction.5 In that case, as in ours, neither patient had a gynecologic pathology. However, in the case presented by Franklin, there was oncologic indication that merited radical dissection. In the City of Hope Hospital in California,6 4 right hemicolectomies with successful transvaginal specimen extraction were performed, in which there was only one internal hernia with bowel obstruction secondary to the defect in the mesenterium.
Palanivelu et al.7 reported on 7 proctocolectomies with ileoanal reservoir due to adenocarcinoma of the upper rectum and coexisting familial polyposis. In these patients, posterior colpotomy and specimen extraction with an endobag were performed. There were complications in 3 of the cases: pouchitis, deep vein thrombosis, and postoperative ileus. Our patient did not present with complications. The mean surgery duration for Palanivelu was 222minutes and in City of Hope, 248minutes; in our case, the procedure took 181minutes. In the study on laparoscopic-assisted total colectomies performed at the Universidad Católica, the patients were released on the 7th postoperative day. Our patient was released on the 3rd day.
The incidence of hernias in traditional laparoscopic colorectal surgery is approximately 17% and of surgical site infection, 10%.8,9 The NOSE modality eliminates these probable complications. In a systematic review of 130 cases, one recto-vaginal fistula and pelvic seroma were reported, with a complication rate under 3%. In addition the NOSE technique was shown to result in a faster recovery of intestinal activity and the use of fewer analgesics. It also required shorter hospital stay, compared with the conventional laparoscopic technique.10 This procedure is an alternative option in the treatment of colonic inertia. Prospective studies are still needed that evaluate its mid and long-term efficacy compared with conventional surgical methods; however, in the 2-year postoperative follow-up, our patient has not presented with any immediate or posterior complications.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Rodríguez-Zentner H, Juárez H, Ríos J, Cáceres M, López JC. Colectomía total con extracción transvaginal del espécimen por inercia colónica. Revista de Gastroenterología de México. 2014;79:153–154.

