
Endoscopic retrograde cholangiopancreatography (ERCP) is a widely performed procedure for the treatment of choledocholithiasis, and more than 90% of bile duct stones can be removed endoscopically.1 Biliary lithotriptors are commonly used to capture and extract the stones, as well as for the performance of mechanical lithotripsy.2
Failure of mechanical lithotripsy can occur when there is a discrepancy between the size of the bile duct stone and the diameter of the distal bile duct,3 or if the stone is large (>10mm) and hard.4 Possible complications are impaction of the stone extraction basket, rupture of the traction wire or the main operation wire, malfunction of the mechanical lithotriptor crank handle, or ductal injury, which occur in 0.6–5.9% of procedures.5
Rapid removal of an impacted biliary stone extraction basket is obligatory to avoid injury to the bile ducts or the intestine. Endoscopic success is achieved in more than 94% of mechanical lithotripsy procedures5 but surgical intervention is necessary in some patients.2–5
We describe herein 3 cases in which an impacted stone extraction basket was retrieved.
Case 1A 64-year-old man was admitted to the hospital with jaundice, upper abdominal pain, and nausea. Abdominal computed tomography revealed situs inversus totalis and a large bile duct stone. ERCP was performed with a 180° rotation of the duodenoscope in the second portion of the duodenum, and cholangioscopy revealed 3 giant stones in the common bile duct (the largest measuring 27mm) (Fig. 1A). Mechanical lithotripsy was attempted but was complicated by a traction wire fracture. Rescue-retrieval forceps were used to dislodge the basket-stone complex, the impacted mechanical lithotriptor was removed uneventfully, and a bile duct plastic stent was placed. Three days later, intraductal cholangioscopy utilizing the SpyGlass® DS system (Boston Scientific Inc., Marlborough, Massachusetts, USA) and laser lithotripsy were successfully performed.
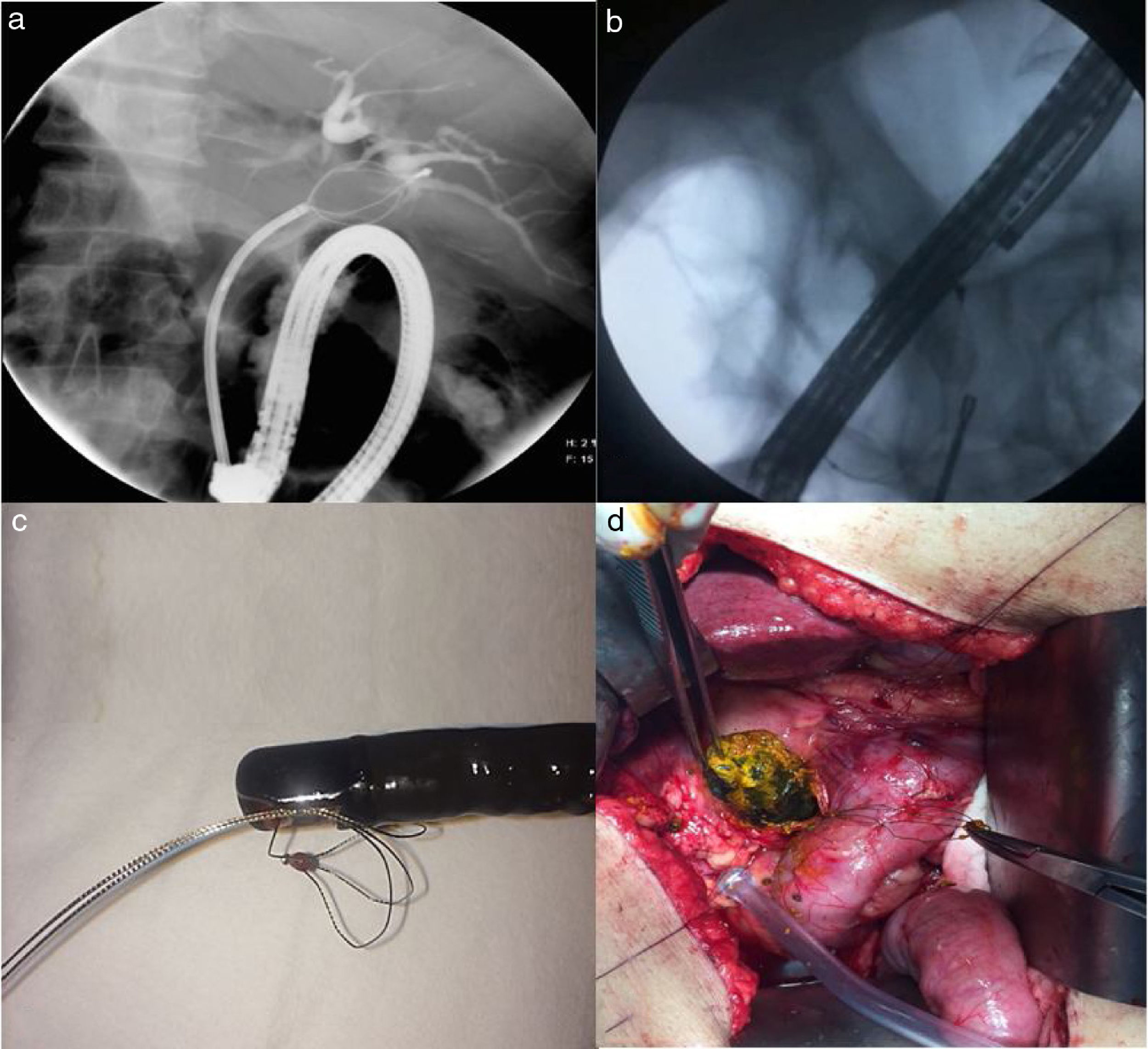
 A cholangiography image showing a stone captured with the biliary stone extraction basket in a patient with situs inversus totalis (case 1). B) A cholangiography image showing the rescue-retrieval forceps used for removing the biliary stone extraction basket (case 2). C) Photograph of the biliary stone extraction basket after removal from the patient (case 2). D) Photograph of the surgery being performed on a patient with an impacted biliary stone extraction basket.")
A) A cholangiography image showing a stone captured with the biliary stone extraction basket in a patient with situs inversus totalis (case 1). B) A cholangiography image showing the rescue-retrieval forceps used for removing the biliary stone extraction basket (case 2). C) Photograph of the biliary stone extraction basket after removal from the patient (case 2). D) Photograph of the surgery being performed on a patient with an impacted biliary stone extraction basket.
A 64-year-old man was initially evaluated at a different hospital for jaundice of one-week progression. Abdominal computed tomography showed a dilated intrahepatic bile duct and extrahepatic common bile duct secondary to a 13mm stone. ERCP was attempted and failed, and a bile duct stent was placed. The patient was referred to our hospital for definitive management. ERCP was performed, and the stent was removed with a snare. Cholangiography revealed a large stone in the common bile duct. After maximal sphincterotomy and biliary balloon dilatation, attempts to clear the stone with a balloon catheter failed. A mechanical lithotriptor basket was advanced, and the stone was captured. The stone could not be pulled out of the bile duct into the duodenum, and the basket traction wire fractured near the handle. Soehendra® mechanical lithotripsy was attempted, and another traction wire fracture occurred. The stone-lithotriptor complex became stuck in the common bile duct. The proximal piece of the basket was then grasped with a pair of rescue-retrieval forceps and successfully removed (Fig. 1B and C, Appendix B supplementary video: demonstration of the recovery of the impacted biliary stone extraction basket, utilizing a rescue-retrieval forceps). The ERCP process was completed with the insertion of a plastic biliary stent. At the follow-up ERCP one week later, the plastic stent and the stone had spontaneously passed out of the bile duct.
Case 3A 66-year-old woman was referred to our hospital due to intermediate risk of choledocholithiasis. An endoscopic ultrasound study identified intrahepatic and extrahepatic bile duct dilatation, associated with multiple stones in the common bile duct. An ERCP was attempted. Cholangiography revealed multiple stones, the largest of which had a diameter of 32×65mm. Sphincterotomy with balloon sphincteroplasty was performed. Seven stones were pulled into the duodenum with a balloon catheter. Biliary extraction basket lithotripsy was attempted for the largest stone, but failed, becoming impacted in the bile duct. Soehendra® mechanical lithotripsy was attempted but was complicated by a traction wire fracture, making extraction impossible. After covering the metallic sheath with a plastic one, the patient was sent to surgery for lithotriptor extraction (Fig. 1D).
Basket impaction is an uncommon but recognized complication of ERCP stone extraction, and is a medical emergency.3 The usefulness of certain maneuvers to retrieve baskets is anecdotal. Some successful techniques have been the use of a Soehendra® mechanical lithotriptor, extracorporeal shock-wave lithotripsy,2 traction with biopsy forceps,6 endoscopic intracorporeal electrohydraulic shock-wave lithotripsy,1 endoscopic laser lithotripsy,7 post-cut technique with a needle knife,8 “flipping the tip” of an impacted basket with a second basket, the use of rat-tooth forceps, and stenting the fractured wire outside the mouth with shorter metal sheaths.3,4
Those salvage methods are not always successful. A watchful waiting strategy can be employed in some cases, after providing biliary drainage or management through a percutaneous transhepatic approach,9,10 whereas other patients will end up in the operating room.10 Such cases are a therapeutic challenge. To the best of our knowledge, the case of the successful removal of the impacted biliary stone extraction basket utilizing rescue-retrieval forceps with no complications in the patient with situs inversus totalis, despite the technical difficulty due to said anatomy, is the first to be reported. The second case was resolved in the same manner. Surgery may be the only option after failed rescue lithotripsy, when there are no other available possibilities for stone extraction, as occurred with our third patient.
Regardless of the technique employed, extraction procedures present a risk of bleeding and perforation, as well as exposure to a higher dose of fluoroscopic radiation, and their successful performance depends on the expertise of the endoscopist.2,8
Ethical disclosureWritten statements of informed consent were obtained from all patients for the performance of the procedure.
Given the study design, approval by an ethics committee was not required.
No confidential patient information appeared in the present article.
Financial disclosureNo financial support was received in relation to the present article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Tepox-Padrón A, Romano-Munive F, Ramírez-Polo AI, Téllez-Ávila FI. Tres reportes de caso de canastilla de extracción de cálculo biliar impactada. Revista de Gastroenterología de México. 2020;85:222–224.

