
The causes of gastrointestinal bleeding of obscure origin (GIBOO) are frequently located in the small bowel, and therefore both capsule endoscopy and double-balloon enteroscopy (DBE) can be used for identifying its etiology.
Pyogenic granuloma (PG) is an inflammatory vascular tumor that typically affects the oral cavity and skin. Digestive system involvement is a rare cause of GIBOO. We present herein a case of PG diagnosed and treated through DBE.
A 71-year-old woman had a past history of type 2 diabetes mellitus (metformin), chronic obstructive pulmonary disease (aerosol bronchodilators), congestive heart disease (hydrochlorothiazide), and coronary disease (isosorbide mononitrate). She sought medical attention for anemia of 8-month progression with no apparent bleeding. She received oral iron treatment with no response and required numerous hospitalizations for blood transfusions.
Upper gastrointestinal video endoscopy and video colonoscopy with intubation of the terminal ileum were normal. Serology for celiac disease was negative, the same as the gynecologic studies. Peripheral blood tests showed microcytic and hypochromic anemia.
Within the context of GIBOO, the decision was made to perform capsule endoscopy to study the small bowel. It had no positive findings and was considered an incomplete study reporting prolonged small bowel transit time.
Given the persistent anemia, lack of response to treatment, and the need for transfusions, the patient was referred to our Service for anterograde DBE.
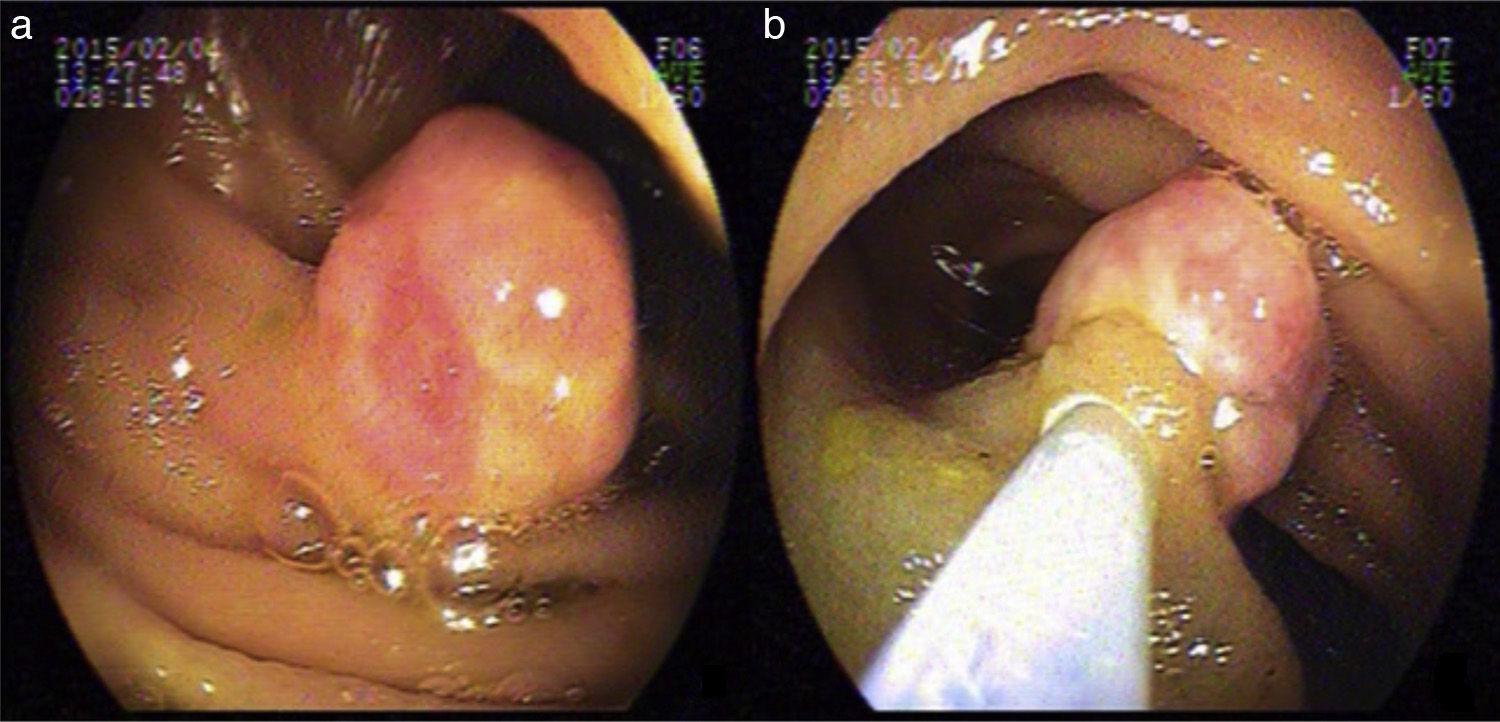
During the procedure, 250cm of small bowel were examined and a 15mm sessile lesion covered with eroded pink mucosa was visualized 150cm from the angle of Treitz. It was resected with a hot snare (after injection of the base with 1/20000 adrenaline) (fig. 1).
 Jejunal lesion 15mm in diameter, and b) Injection at the base of the lesion.")
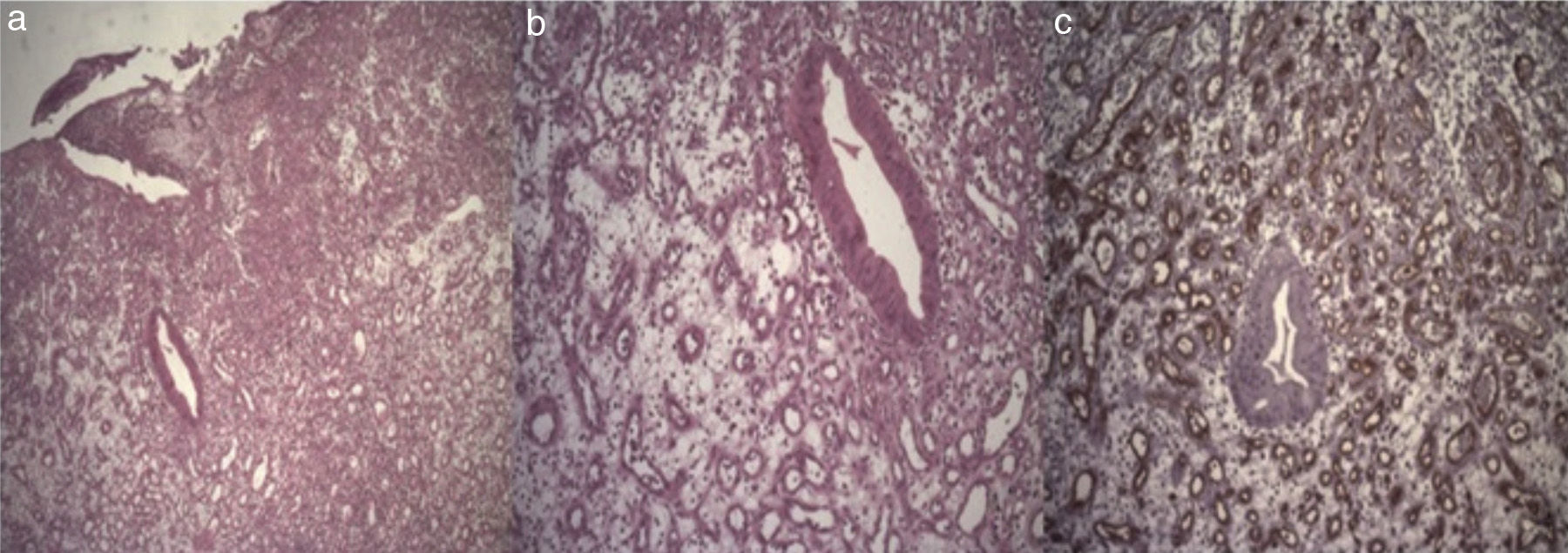
The histology study reported a polypoid formation with an epithelium with an ulcerated surface and edematous stroma with dense mixed inflammatory infiltrate accompanied by numerous neoformation vessels, scant cryptic structures with dense cellular cytoplasm, and nuclei with marked reactive changes. CD34 stain was positive for blood vessels and the diagnosis was intestinal PG. The resection margins were lesion-free (fig. 2).
, x100, (b) and marked with CD34 (c). Capillaries and vascular proliferation marked with dense mixed inflammatory infiltrate.")
After 8 months of follow-up, the patient progressed with stable hematocrit and no need for transfusion.
GIBOO is defined as gastrointestinal tract bleeding that persists or recurs with no obvious etiology after the performance of 2 gastrointestinal endoscopies (upper and lower). Capsule endoscopy enables the site of bleeding to be located and thus defines the entrance pathway of the DBE (anterograde or retrograde). DBE is a very effective therapeutic tool in the management of small bowel pathologies.1–3 Capsule endoscopy provided no results in our patient and the diagnosis and treatment were established through the anterograde DBE.
PGs, also known as lobular capillary hemangiomas, are benign vascular tumors of the skin and mucosae that rarely involve the digestive system.4–7 Their pathophysiology implies mechanical damage. The etiology of GPs of the small bowel is unknown, unlike those located in the oral cavity and esophagus, which are presumed to be associated with damage to the mucosal layer due to foods, Barrett's esophagus, or gastroesophageal reflux.8 Endoscopically, they appear as small, pink polyps, with a wide base and ulcers smaller than 3cm in diameter. Some of them can bleed.6 The endoscopic characteristics found in our patient coincided with those reported in previous studies.
PG can originate in the mucosa or submucosa, appearing as an infiltrate of inflammatory cells and vascular proliferation.8
Given that these lesions are a cause of GIBOO and do not regress spontaneously, they should be treated endoscopically2 or through surgery.3,4,7
The anatomopathologic report of our case described complete lesion resection, including the arteriovenous anastomosis underlying the PG, which minimizes the recurrence of lesions associated with partial extractions.
Nagoya et al. reported a case of endoscopic resection in the ileum with DBE. However, they could not determine whether the vertical margins of the resection were negative.2
Nakaya et al. described persistent bleeding after biopsy and therefore its performance should be carefully considered.9
PG of the gastrointestinal tract is a rare condition and fewer than 30 cases have been published up to the present.1–10 We believe that endoscopic polypectomy is a feasible treatment option, but because they are highly vascularized structures, the risk for bleeding at the time of extraction must be considered and additional measures of endoscopic hemostasis contemplated, such as adrenaline injection, clipping the base of the lesion, or thermal methods.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
The authors wish to thank the Research Area of the Hospital “El Cruce” Dr. Néstor Carlos Kirchner, and in particular the physicians Maximiliano De Abreu and Laura Antonietti for their collaboration in preparing this manuscript.
Please cite this article as: De María J, Curvale C, Guidi M, Hwang H, Matanó R, Granuloma piógeno de yeyuno. Diagnóstico y tratamiento con enteroscopia doble balón. Reporte de un caso. Revista de Gastroenterología de México. 2017;82:94–96.

