
When the etiologic differential diagnosis is made in immunocompromised patients with chronic diarrhea, human intestinal spirochetosis (HIS) is never, or hardly ever, considered. In addition to being a rare cause, HIS is a trying challenge for the physician, given the absence of pathognomonic clinical and laboratory variables. This situation results in lowering the probability of its diagnosis prior to intestinal biopsy interpretation, as well as making active searching for the disease less likely. Unlike the few reports identified in databases available in the literature, ours is a clinical case describing this pathology from an endoscopic and histopathologic approach.
HIS is morphologically defined by the presence of spirochetes adhered to the apical membrane of epithelial cells of the colon and rectum.1 Intestinal spirochetosis is a frequent cause of outbreaks of diarrhea in poultry, dogs, and sheep, but in humans, the Brachyspira aalborgi and Brachyspira pilosicoli species are pathogenic. The incidence and prevalence of diarrhea caused by said pathogens has been estimated at 0.4–12%.2 Infection is more frequent in men, especially in homosexual males practicing unsafe sex, in HIV-positive men regardless of their sexual orientation or degree of immunodeficiency, and in men from low-income areas with poor sanitation.3,4 The clinical presentation of HIS is chronic watery diarrhea, abdominal pain and/or hematochezia. However, some patients are asymptomatic and are diagnosed incidentally when colonic biopsies are evaluated for other reasons,5 which has opened the debate on whether intestinal spirochetosis is a pathogen or a commensal microbe.6 The endoscopic appearance of the colon is nonspecific and its description ranges from normal characteristics to “polypoid” lesions and irregular erythematous patches, which in the majority of cases are the indication for biopsy. This involvement can extend from the proximal to the distal colon, including the rectum, and in anecdotal cases, the cecal appendix.7 Histopathologic study traditionally reports a diffuse blue fringe through hematoxylin and eosin staining along the border of the intercryptal epithelial layer; said finding is known as the “false brush border”.8 Once the infection is suspected, Warthin-Starry or Dieterle silver stains can be used to highlight the spirochetes in fixed tissue.1 Very little has been described in the literature about the antimicrobial management of patients with HIS. Some patients have complete remission of diarrhea and normalization of the colorectal mucosa, whereas others continue to be symptomatic, with or without the “false brush border”. In general, an antibiotic therapy regimen is justified, more frequently with metronidazole, for a course varying from 7 to 10 days.9 Other case reports have shown symptom resolution with the use of clindamycin and certain macrolides.4,10 We present herein the case of a 47-year-old man, with a past medical history of HIV positivity (WHO A2 subtype) and autoimmune hepatitis overlapping with primary biliary cholangitis (PBC), receiving antiretroviral therapy (ART), whose present illness had a clinical picture of 4-month progression of watery chronic diarrhea, associated with generalized colicky abdominal pain and intermittent episodes of hematochezia. Total colonoscopy revealed ulcerated segmental colitis of the left colon and transverse colon and a Paris 0-1 pedunculated lesion (NICE 2) in the left colon (Fig. 1). Biopsy samples were taken of the polypoid and ulcerated lesion and sent to the pathology laboratory; intestinal spirochetosis was reported (Fig. 2). The patient was treated with 500 mg of oral metronidazole every 12 h for 10 days, with complete symptom resolution.
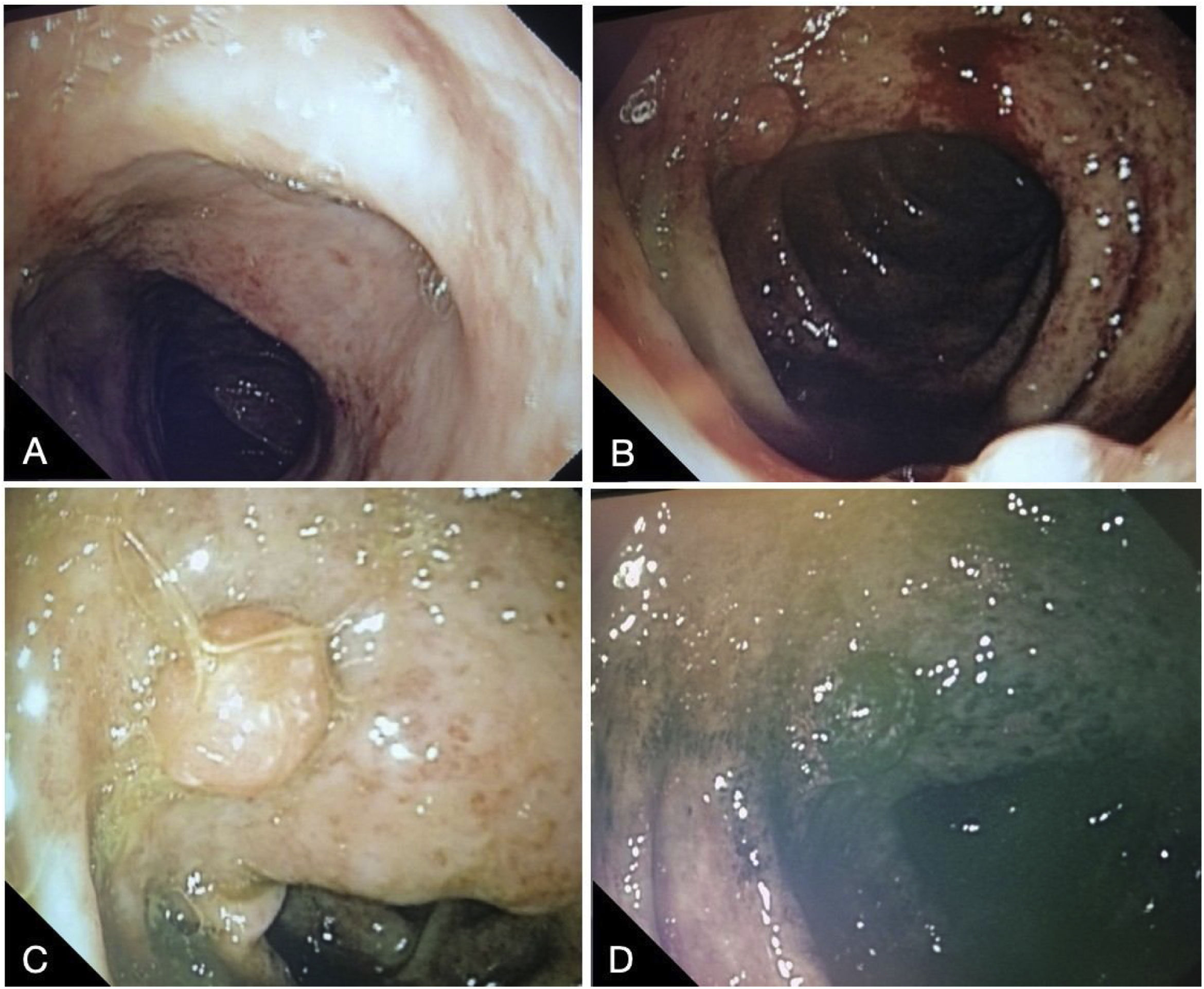
 Transverse colon: diffuse erosions with vascular pattern loss and disperse fibrin-covered ulcerations measuring 2 mm. B–D) Left colon: Diffuse erosions with vascular pattern loss, with dispersed 2 mm fibrin-covered ulcerations, can be seen at the most distal part of the left colon. A hyperchromic 11 mm sessile polypoid lesion, with a superficial trabecular pattern and regular vascular pattern, can be seen on chromoendoscopy-narrow band imaging (NBI).")
Total colonoscopy finding ulcerated segmental colitis of the left colon and transverse colon, associated with polypoid lesions in the left colon. A) Transverse colon: diffuse erosions with vascular pattern loss and disperse fibrin-covered ulcerations measuring 2 mm. B–D) Left colon: Diffuse erosions with vascular pattern loss, with dispersed 2 mm fibrin-covered ulcerations, can be seen at the most distal part of the left colon. A hyperchromic 11 mm sessile polypoid lesion, with a superficial trabecular pattern and regular vascular pattern, can be seen on chromoendoscopy-narrow band imaging (NBI).
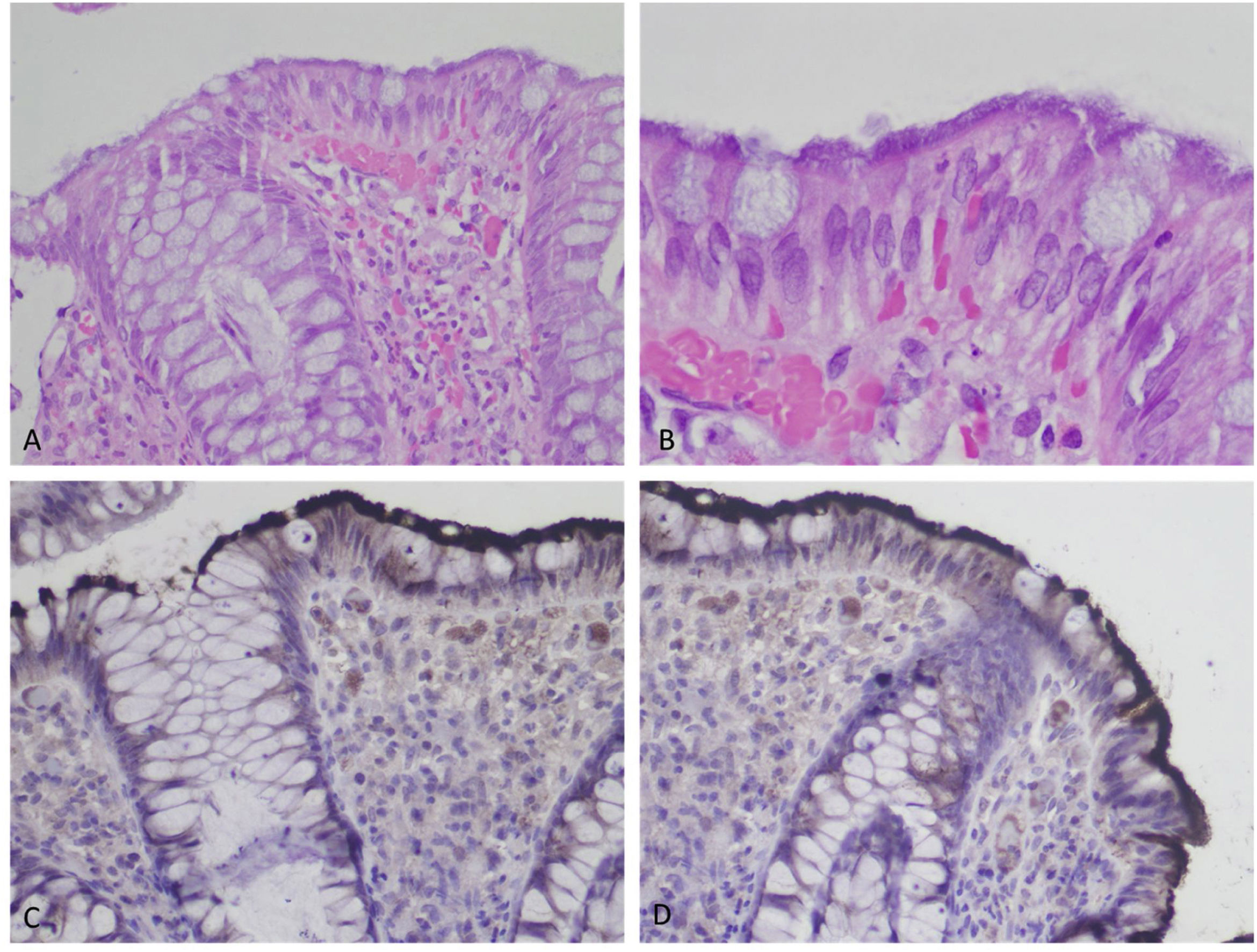
 Colonic mucosa with nonspecific lymphocytic infiltrate in the lamina propria on the blurry surface (×10, H&E). B) Mucosal surface with a brush border aspect (x100, H&E), hematoxylin and eosin stain. C, D) Immunohistochemical staining for treponema highlights the spirochetes on the epithelial surface (×40).")
Biopsy of the colonic mucosa taken at endoscopy. A) Colonic mucosa with nonspecific lymphocytic infiltrate in the lamina propria on the blurry surface (×10, H&E). B) Mucosal surface with a brush border aspect (x100, H&E), hematoxylin and eosin stain. C, D) Immunohistochemical staining for treponema highlights the spirochetes on the epithelial surface (×40).
HIS should be actively looked for in patients with chronic diarrhea, especially those presenting with immunosuppression. We have found very few case reports on the condition and the majority of cases have been incidental findings. The present case report brings together important elements for learning more about HIS, given that it provides a complete description of a diarrheic syndrome in an immunosuppressed patient, with nonspecific findings in colonoscopy, but an active histopathologic search for spirochetes, once the most frequent pathologies were ruled out. According to the timeline of events, the patient’s symptoms were resolved after he received antimicrobial treatment, concurring with results published in previous reports. We were struck by the finding of polypoid lesions in the colon. They have been described as a recurrent finding in some of the reports in the literature, but so far, lacking an explanation. Determining whether there is biologic feasibility and causality is something well worth studying. A limitation of our report is the fact that we could not directly evaluate the effect of treatment histopathologically, given that the patient was lost to follow-up.
HIS is a rare cause of chronic diarrhea in immunocompromised patients. Because there are no pathognomonic clinical or laboratory variables, it should be included in the differential diagnosis; another fundamental aspect for its diagnosis is having an experienced pathology team that can look for spirochetes in samples obtained endoscopically.
Ethical considerationsThe present work did not require approval by the Bioethics Committee of the Pontificia Universidad Javeriana because, in accordance with the ethics guidelines of the Council for International Organizations of Medical Sciences (CIOMS version 2016) for human health research, it is considered low-risk research. The patient signed a written statement of informed consent. We declare that this article contains no personal information that could identify the patient.
Financial disclosureNo specific grants were received from public sector agencies, the business sector, or non-profit organizations in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Chaar AJ, Arbelaez JS, Vargas MJ, Cañadas RA. Espiroquetosis intestinal humana como causa de diarrea crónica en un paciente VIH positivo: reporte de caso. Rev Gastroenterol Mex. 2023;88:443–446.

