
Gastric cancer is the second cause of death by cancer worldwide. Histologic classification may predict tumor biology, clinical behavior, and outcome. According to the Lauren classification, the disease is divided into 2 types, diffuse and intestinal, and the latter has a better prognosis.
AimTo determine the frequency of gastric adenocarcinoma and compare the histopathologic characteristics of intestinal and diffuse-type gastric adenocarcinoma in Mexican patients treated at a tertiary referral hospital.
MethodologyA retrospective study evaluated the pathology reports of patients with gastric adenocarcinoma corresponding to the time frame of January 2003 to December 2012. Adenocarcinomas of the gastric cardia were excluded. Frequencies were expressed as percentages and the categorical variables were compared with the chi-square test. Statistical significance was set at a P<.05.
ResultsA total of 417 cases of gastric adenocarcinoma were found, 230 (55.2%) of which were diffuse-type and 118 (28.2%) were intestinal-type. The mean age of the patients with diffuse type gastric cancer was 54.02±14.93 and 119 (51.3%) of those patients were men. The mean age of the patients with intestinal-type gastric cancer was 63.43±13.78, and 69 (62.2%) were men. Ninety-two of the diffuse-type patients were under the age of 50 years, compared with 22 of the patients with intestinal-type carcinoma.
ConclusionsThis is the first study on the Mexican population to analyze the differences in the histologic types of adenocarcinoma. Diffuse-type gastric carcinoma was the most frequent subtype in our study population and it is associated with worse outcome.
A nivel mundial el cáncer gástrico es la segunda causa de muerte. La clasificación histológica puede predecir la biología del tumor, el comportamiento clínico y el pronóstico. De acuerdo a la clasificación de Lauren, se divide en tipo difuso e intestinal. El tipo intestinal muestra mejor pronóstico que el tipo difuso.
ObjetivoDeterminar la frecuencia de adenocarcinoma gástrico y comparar las características histopatológicas de los subtipos de adenocarcinoma gástrico intestinal y difuso en pacientes mexicanos tratados en un centro de referencia de tercer nivel.
MetodologíaEstudio retrospectivo en el que se evaluaron informes patológicos de pacientes con adenocarcinoma gástrico de enero del 2003 hasta diciembre del 2012. Se excluyeron los adenocarcinomas del cardias. Las frecuencias se expresaron con porcentajes y las variables categóricas se compararon con la prueba de ji cuadrado. Los valores de p<0.05 se consideraron como significativos.
ResultadosSe encontraron 417 casos de adenocarcinoma gástrico. Hubo 230 (55.2%) con tipo difuso y 118 (28.2%) con tipo intestinal. La edad media en el tipo difuso fue 54.02±14.93 años de los cuales 119 (51.3%) fueron hombres, y la de tipo intestinal fue 63.43±13.78, y 69 (62.2%) fueron hombres. Entre el carcinoma de tipo difuso, 92 fueron menores de 50 años en comparación con 22 con carcinoma de tipo intestinal.
ConclusionesEste es el primer estudio en nuestra población que hace diferencias entre los tipos histológicos del adenocarcinoma. El subtipo de adenocarcinoma gástrico más frecuente en nuestra población fue el difuso, el cual se asocia a peor pronóstico.
Gastric cancer is the second cause of death by cancer worldwide.1 In 2012, the World Health Organization estimated about one million new cases of gastric cancer (952,000 cases, 6.8% of all cancers), putting it in fifth place for malignant neoplasias, after lung, breast, colorectal, and prostate cancers; more than 70% of the cases (677,000 cases) occurred in developed countries (456,000 cases in men; 221,000 in women) and half of those cases were on the Asian continent (mainly China)2
For the year 2011 in Mexico, gastric cancer was among the main causes of hospital morbidity in men, with the highest rate in the 75 to 79-year-old population (47 of every 100,000 men in that age group), followed by the 65 to 74-year-old population (38 of every 100,000 men of that age group). It is currently known that of the main malignant tumors causing death in the Mexican population of 20-year-olds, gastric cancer is the 3rd cause in both women (7%) and men (8.6%), after breast cancer (13.8%), cervical cancer (10.4%), prostate cancer (16.9%), and bronchial/lung cancer (12.8%), respectively.3
According to Lauren, gastric adenocarcinoma is a heterogeneous disease that is histologically divided into the intestinal, diffuse, and undifferentiated non-mucus-producing types,4 and is anatomically classified as proximal or distal.5 More recently, genomic and molecular classifications have been made,6–8 and numerous molecular alterations may be involved in each histologic subtype. Anatomic and histologic classification can provide knowledge about tumor biology and facilitate the selection of a population to receive targeted therapies.9
Gastric cancer development is a multifactorial and complex process with a lengthy progression. It is very unlikely that infection by Helicobacter pylori alone is responsible for the development of gastric cancer. There is evidence that the consumption of salty foods, N-nitroso compounds, and a low consumption of fresh fruit and vegetables increase the risk for gastric cancer.10
Intestinal-type adenocarcinoma is associated with severe atrophic chronic gastritis, intestinal metaplasia, and dysplasia. It corresponds to well or moderately differentiated carcinomas, and is characterized by the formation of glandular cells similar to intestinal cells. It is mainly situated in the antrum and settles in zones of previous intestinal metaplasia, especially of the colonic or incomplete type.11 Diffuse-type adenocarcinoma encompasses the infiltrative variety and is poorly differentiated, with the presence of signet ring cells and without apparent gastritis. It is thought to appear de novo and is associated with low CDHI regulation.12 There are no epidemiologic studies on the Mexican population that classify gastric adenocarcinoma by histologic subtype, in the knowledge that each subtype behaves differently.
The aim of this study was to determine the frequency of gastric adenocarcinoma and compare the histopathologic characteristics of its subtypes reported at the Hospital Juárez de México (a tertiary care center) over the last 10 years.
MethodsPatientsA retrospective and confidential database was elaborated in relation to all the patients with gastric adenocarcinoma diagnosed within the time frame of January 2003 and December 2012 at the Hospital Juárez de México. Histologic confirmation was performed by the hospital's Pathology Department. Other tumors, such as lymphomas, sarcomas, and neuroendocrine, gastric cardia, and gastroesophageal junction tumors were excluded from the analysis. The study included patients above the age of 18 years.
Study designPatient medical records were reviewed to obtain the following data that included age at the time of diagnosis, sex, tumor location (only including those located in the body, antrum, and pylorus), and histologic subtypes based on the Lauren classification. The type of sample (biopsy or gastrectomy) was specified, along with differentiation grade, infiltration grade, and the presence of ulceration, lymph node invasion, perineural and angioinvasion, surgical margins, and Helicobacter pylori.
Statistical analysisA retrospective study was conducted that covered a 10-year time period. The Windows SPSS program was used for the statistical analysis and the continuous variables were expressed as means and dispersion coefficients were used for standard deviation. Frequencies were expressed as percentages and the categorical variables were compared utilizing the chi-square test. Statistical significance was set at a p<0.05.
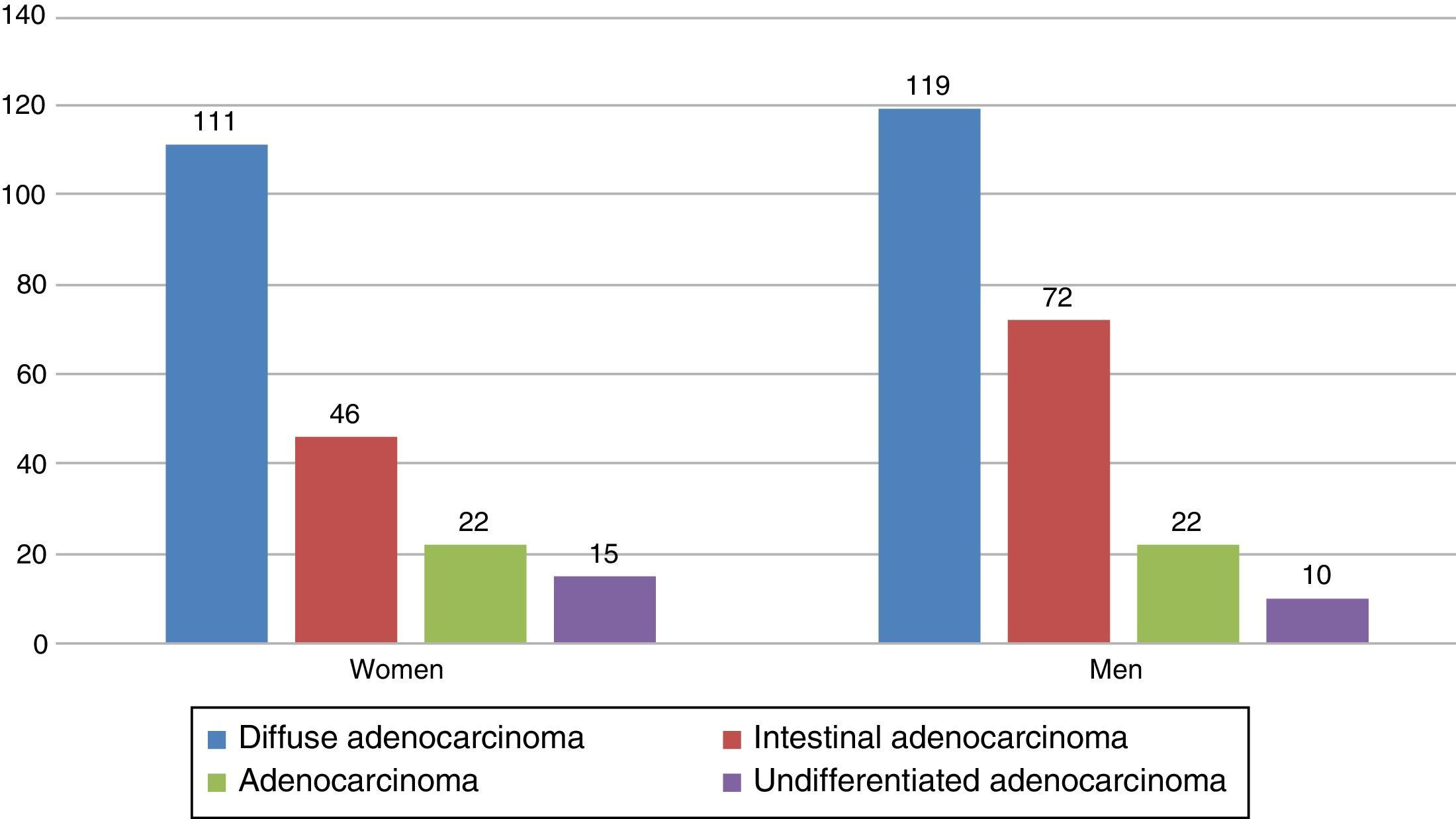
ResultsA total of 417 cases of gastric adenocarcinoma were found. Three hundred and thirty-four (80%) of them were obtained through endoscopic biopsy and 83 (20%) through gastrectomy (51 partial, 26 total, and 6 not specified). Diffuse-type adenocarcinoma was reported in 230 patients (55.2%), intestinal-type in 118 patients (28.2%), and undifferentiated-type in 25 patients (6%); sub-type was not determined in 44 patients (10.6%) (figure 1). The mean age for the diffuse-type patients was 54.02±14.93 and 118 of those patients (51.3%) were men. The mean age for the patients with the intestinal type was 63.43±13.78, and 69 (62.2%) were men.

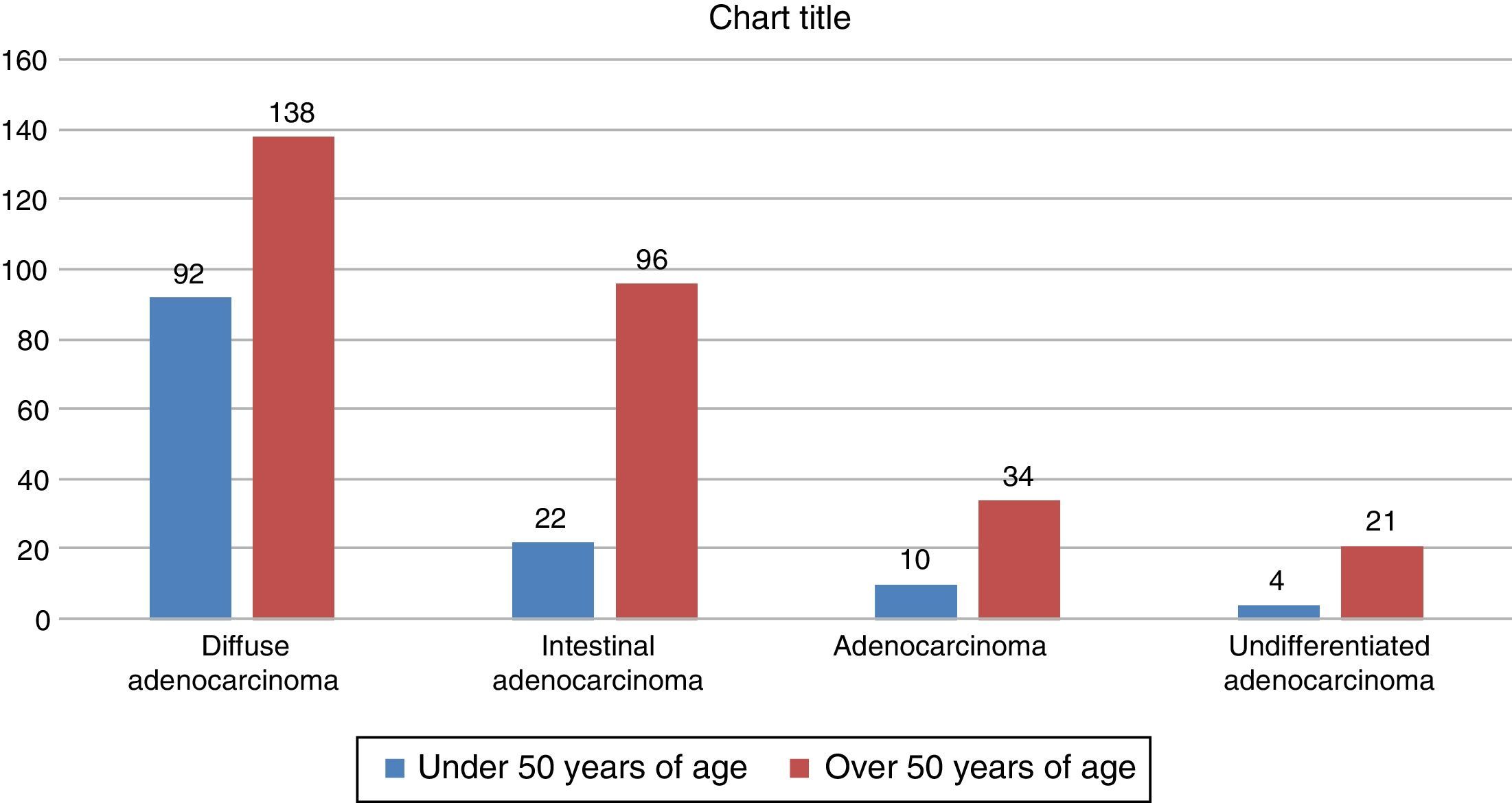
The diffuse type had a statistically significant association in relation to the number of cases in patients < 50 years of age (p<0.001), perineural invasion (p=0.5), positive surgical margins (p<0.5), and positive angioinvasion (p<0.5).
Among the diffuse-type patients, 92 were under 50 years of age, compared with 22 patients with intestinal-type carcinoma (figure 2).
Discussion
Analyzing the histologic subtypes of gastric adenocarcinoma in patients diagnosed over the last 10 years at the Hospital Juárez de México, the diffuse-type was observed to be the most prevalent, presenting in one-third of the patients under 50 years of age.
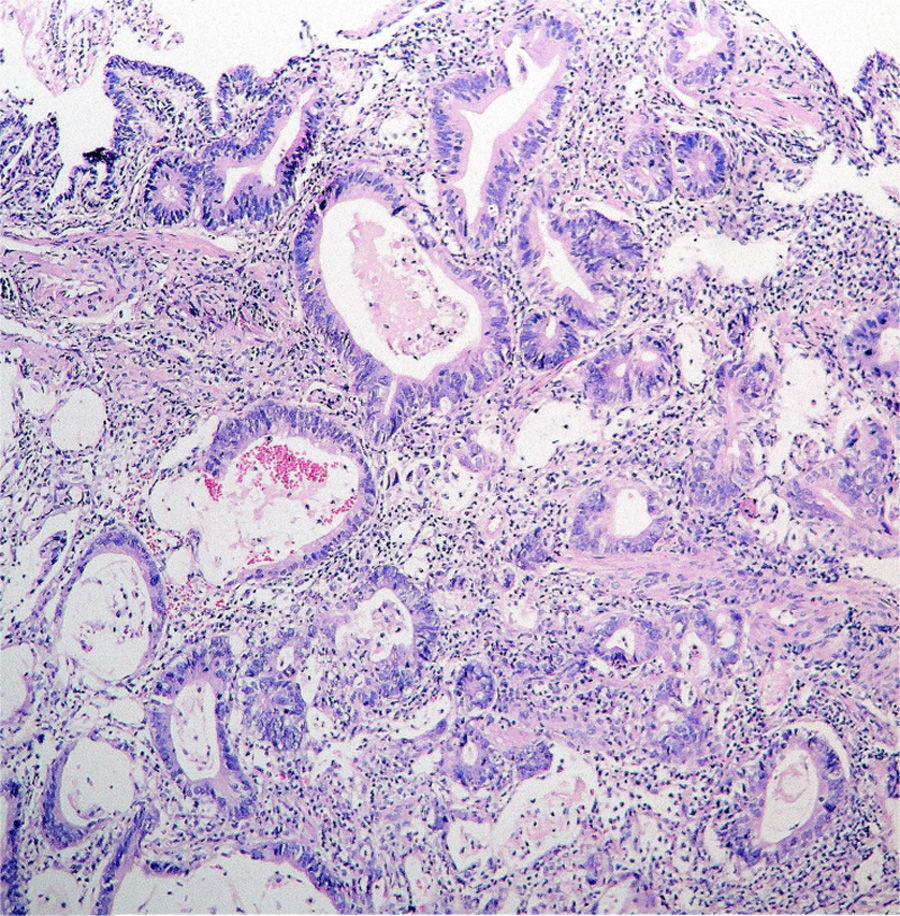
There are no studies in Mexico that classify adenocarcinoma by subtype or anatomic location. In a study by Bonequi et al.,13 they carried out a search of the PubMed database and reported that in 9 out of 20 Latin American countries, including Mexico, the histologic gastric adenocarcinoma subtype encountered was the intestinal-type in the distal location (figure 3). There are high incidence rates of gastric cancer in Latin America, but the reasons for this are not yet known. Convincing data suggest environmental factors and certain diseases, such as atrophic gastritis,14 adenomatous polyps,15 dysplasia,16 metaplasia,17 Ménétrier's disease,18 and pernicious anemia.19 Also included are nutritional factors, such as high salt intake and the consumption of smoked foods, spicy foods, nitrite-rich foods, foods high in carbohydrates and fat, and the low consumption of milk, fresh fruit and vegetables, selenium, and vitamins A, C, and E.20 High tobacco and alcohol consumption as risk factors for gastric cancer are still a subject of debate.21,22

Numerous researchers have reported a worse prognosis for patients with proximal cancer than those with cancer that is located in the mid and distal regions of the stomach.23 Despite the fact that the global incidence of gastric cancer continues to decrease, the incidence of proximal and gastroesophageal junction gastric adenocarcinoma in the U.S. is increasing.24,25
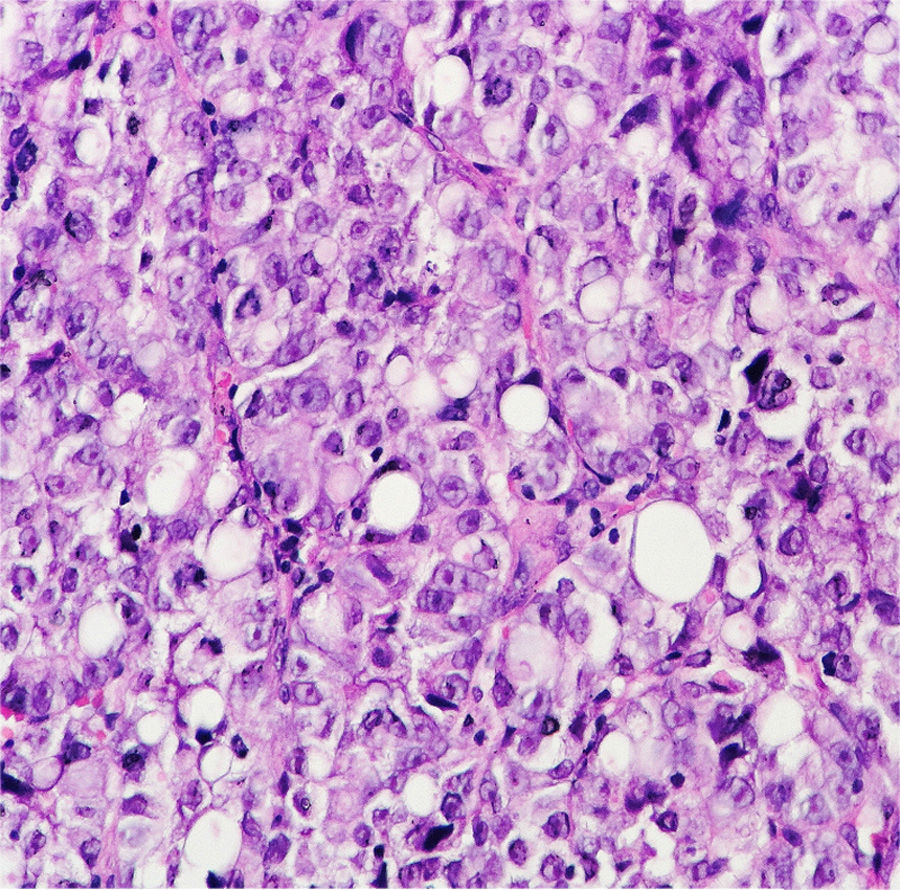
The development of molecular biology has improved our understanding of gastric cancer, even though its molecular mechanisms are not yet known. Some interesting molecules have been suggested as prognostic markers in these patients, including cell adhesion molecules.26 Multiple pathways are involved in different subtypes: human epidermal growth factor receptor 2 (HER2)27 and epidermal growth factor receptor28 overexpression predominate in non-diffuse cancer. Diffuse-type gastric cancer is characterized by aberrant cell adhesion (figure 4). Cadherins, together with catenins, play an important role in cell adhesion and polarity.29 Defects in the APC and DCC genes, microsatellite instability, and promoter hypermethylation of the hMLH1 gene have been associated with intestinal-type gastric cancer.30–33 Tumor suppressing genes, such as p53,34 and overexpression of the epidermal growth factor receptor, vascular endothelial growth factor receptor, and HER2 have all been associated with poor outcome.35,36 Targeted therapies combined with chemotherapy have produced encouraging results in the treatment of patients with advanced esophageal and gastric cancer.37

Patients of different racial and ethnic groups, whatever their origins, have different natural histories, detection and treatment access, as well as dissimilar outcomes, in relation to numerous diseases.38 These variations have an important value because they enable the identification of biologic, environmental, and socioeconomic differences. The understanding of the biologic and molecular basis of gastric cancer can facilitate oncologic therapy adapted to the individual characteristics of each specific tumor.
Ours is the first study on the Mexican population to highlight the differences between the histologic subtypes of gastric adenocarcinoma, which could facilitate the selection of targeted therapies. The most frequent gastric cancer subtype in our population was the diffuse-type, which is associated with worse outcome. Up to one-third of the patients with gastric adenocarcinoma were under the age of 50 years, which has significant economic implications. The histology, sex, and age at time of presentation justify further research on the epidemiology, pathogenesis, and molecular biology of gastric cancer in Mexico.
Ethical responsibilitiesProtection of persons and animalsThe authors declare that no experiments were performed on humans or animals for this study.
Data confidentialityThe authors declare that they have followed the protocols of their work center in relation to the publication of patient data.
Right to privacy and informed consentThe authors have obtained the informed consent of the patients and/or subjects referred to in the article. This document is in the possession of the corresponding author.
Financial disclosureNo financial support was received in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Martínez-Galindo MG, Zamarripa-Dorsey F, Carmona-Castañeda A, Angeles-Labra A, Peñavera-Hernández R, Ugarte-Briones C, et al. Características histopatológicas del adenocarcinoma gástrico en pacientes mexicanos. Experiencia de 10 años en el Hospital Juárez de México. Revista de Gastroenterología de México. 2015;80:21–26.

