
Since the first description of “Downhill” varices,1 or varices in the proximal esophagus, by Felson and Lessure in 1964, there have been only about 80 articles on the theme in the literature. The appearance of this phenomenon in the proximal third of the esophagus arises from obstruction of the blood flow from the superior vena cava, proximal to the azygos vein, forcing the veins to drain through the mediastinal collateral vessels that appear in the proximal esophagus.2–4 Lung cancer, lymphoma, and mediastinal metastases are among the malignant causes of this entity5 and goiter, congenital or valvular heart disease, thymoma, and systemic vasculitides, such as Behcet's disease, are included among its benign causes. These varices can also be secondary to procedures such as pacemaker insertion or hemodialysis access.3,4 Hypercoagulability disorders are another etiology, with one case reported in the literature.2 We describe herein a case of “Downhill” esophageal varices secondary to a hypercoagulability disorder.
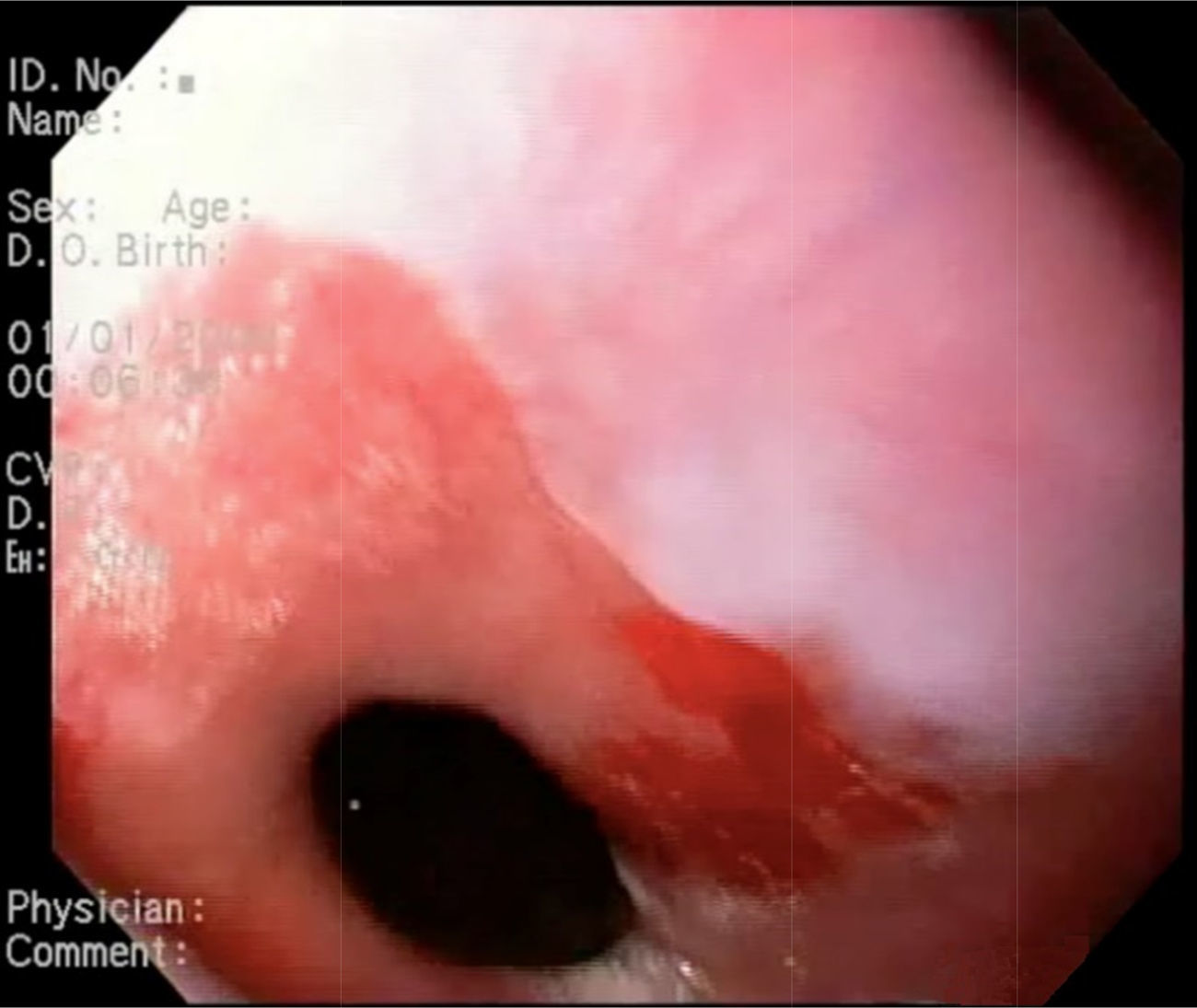
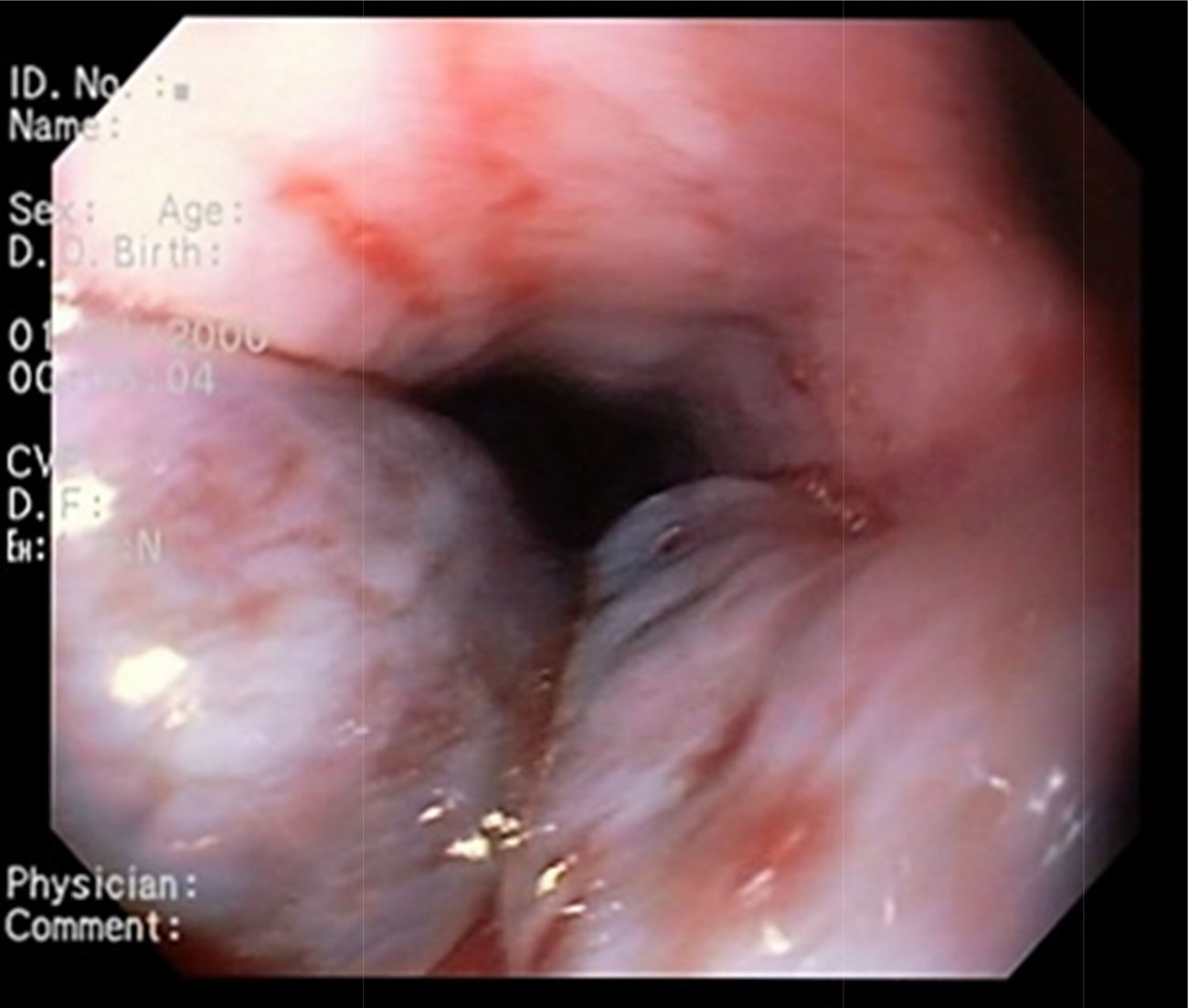
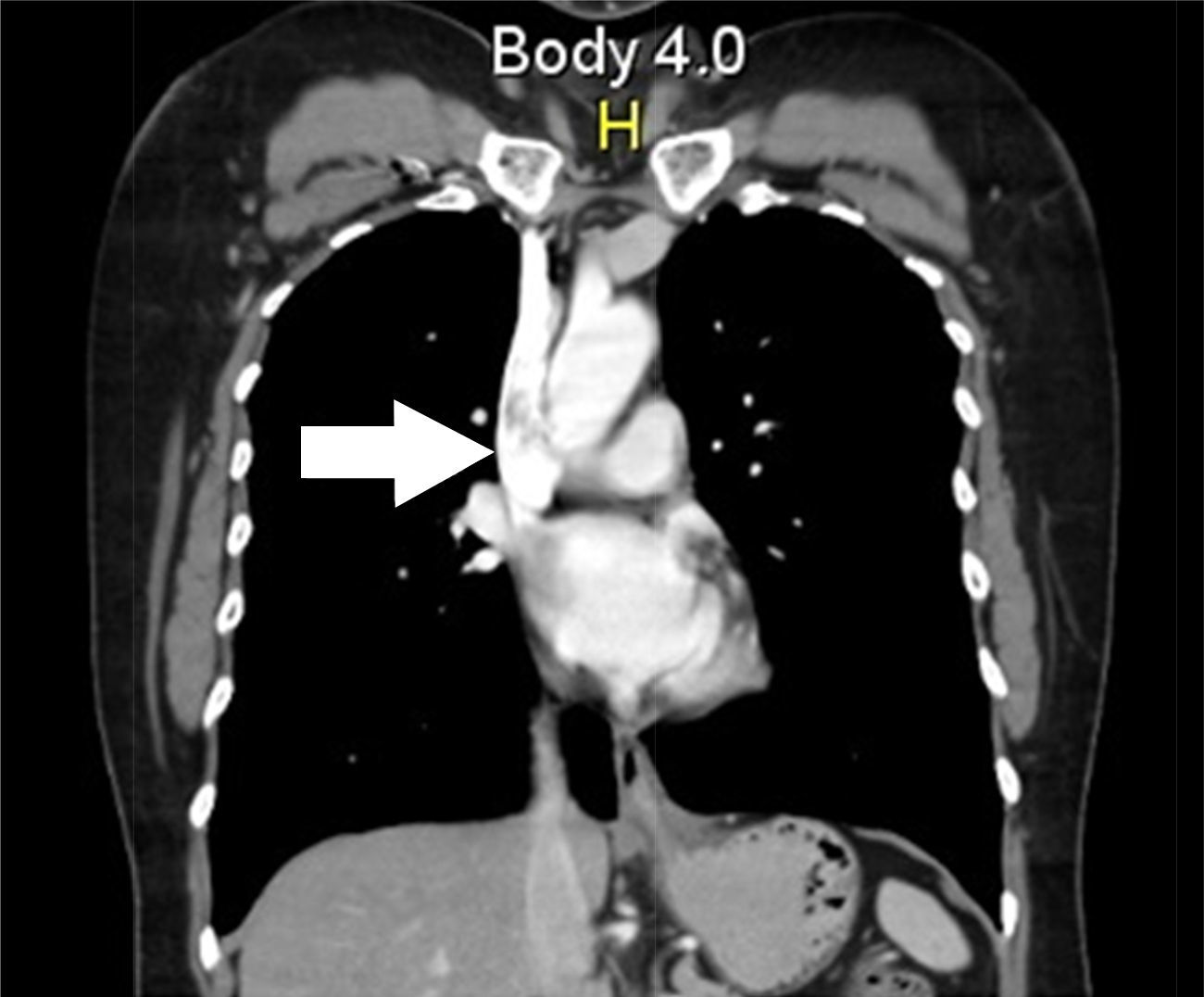
A 53-year-old woman with no remarkable past history was admitted to the emergency department due to hematemesis with no abdominal pain of 2-day progression. Physical examination revealed a heart rate of 90, blood pressure of 100/60, and rectal examination was positive for melena. At endoscopy, an unaltered gastroesophageal junction was observed (fig. 1), as well as 2 venous dilations in the proximal third of the esophagus with no evidence of active bleeding (fig. 2), suggestive of Downhill varices. A computed tomography chest scan showed an image of a thrombus in the superior vena cava (fig. 3). Anticoagulation management was begun with enoxaparin. Control endoscopy was carried out at 72h that revealed a reduction in the size of the esophageal varices. Hypercoagulability studies were begun, with normal results, except for the factor V Leiden mutation.



The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Conflict of interestThe authors declare that there is no conflict of interest.
The authors wish to thank the Universidad Nacional de Colombia for the logistic and diagnostic support received in relation to this case report.
Please cite this article as: Gómez-Aldana AJ, Gómez-Zuleta MA. Varices esofágicas en Downhill secundarias a trombosis de vena cava superior por déficit de factor V. Revista de Gastroenterología de México. 2017;82:179–180.

