


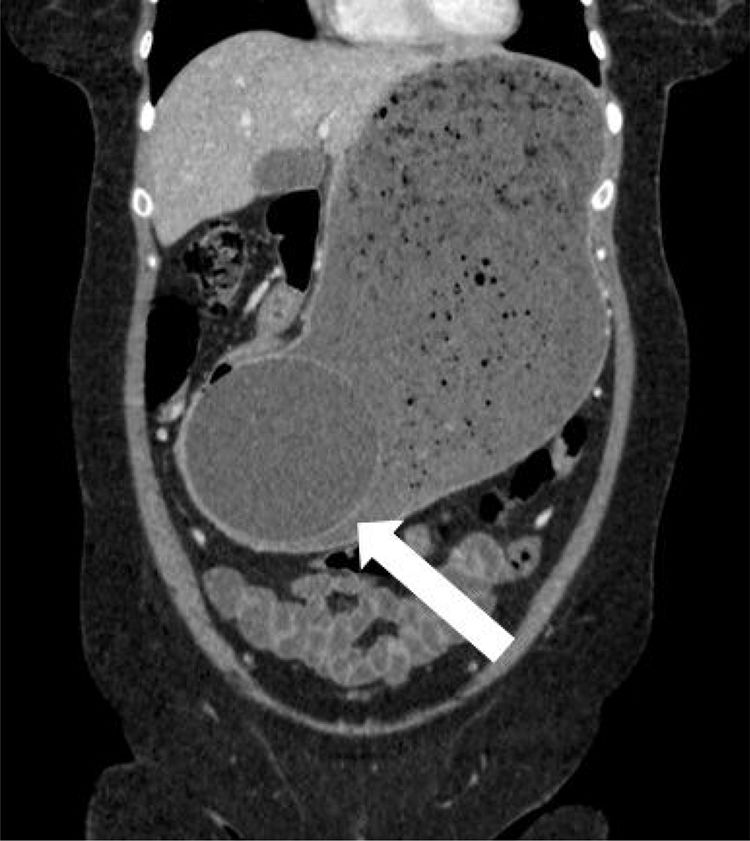
A 45-year-old woman came to the emergency service due to 3 days of ongoing vomiting and significant generalized and progressive abdominal distension. Her past medical history was unremarkable, except for the placing of an intragastric balloon 3 weeks prior. Plain abdominal x-ray revealed an occupied abdomen and bowel loop displacement toward the periphery. A computed axial tomography scan identified severe dilation of the gastric corpus, along with the intragastric balloon (white arrow), which was embedded in the antral region, causing the gastric outlet obstruction (Figure 1 in the axial plane, Figure 2 in the sagittal plane, and Figure 3 in the coronal plane). According to the medical literature, frequency of overall complications from intragastric balloon placement reaches 2.6% and obstruction is one of the most common causes in the early postoperative period, with a frequency of 0.8%. First, a nasogastric tube was placed in our patient to relieve the distension, after which the obstruction was resolved through endoscopic removal of the balloon. After the intervention, the suggested cause was the progression of the balloon and its lodging in the antrum of the stomach, with no excessive filling of that gastric region.



No financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Rubio Solís D, Sánchez García S. Obstrucción gástrica secundaria a balón intragástrico. Revista de Gastroenterología de México. 2018;83:346–347.

