
Acute appendicitis is the first cause of surgical emergencies. It is still a difficult diagnosis to make, especially in young persons, the elderly, and in reproductive-age women, in whom a series of inflammatory conditions can have signs and symptoms similar to those of acute appendicitis. Different scoring systems have been created to increase diagnostic accuracy, and they are inexpensive, noninvasive, and easy to use and reproduce. The modified Alvarado score is probably the most widely used and accepted in emergency services worldwide. On the other hand, the RIPASA score was formulated in 2010 and has greater sensitivity and specificity. There are very few studies conducted in Mexico that compare the different scoring systems for appendicitis. The aim of our article was to compare the modified Alvarado score and the RIPASA score in the diagnosis of patients with abdominal pain and suspected acute appendicitis.
Material and methodsAn observational, analytic, and prolective study was conducted within the time frame of July 2002 and February 2014 at the Hospital Universitario de Puebla. The questionnaires used for the evaluation process were applied to the patients suspected of having appendicitis.
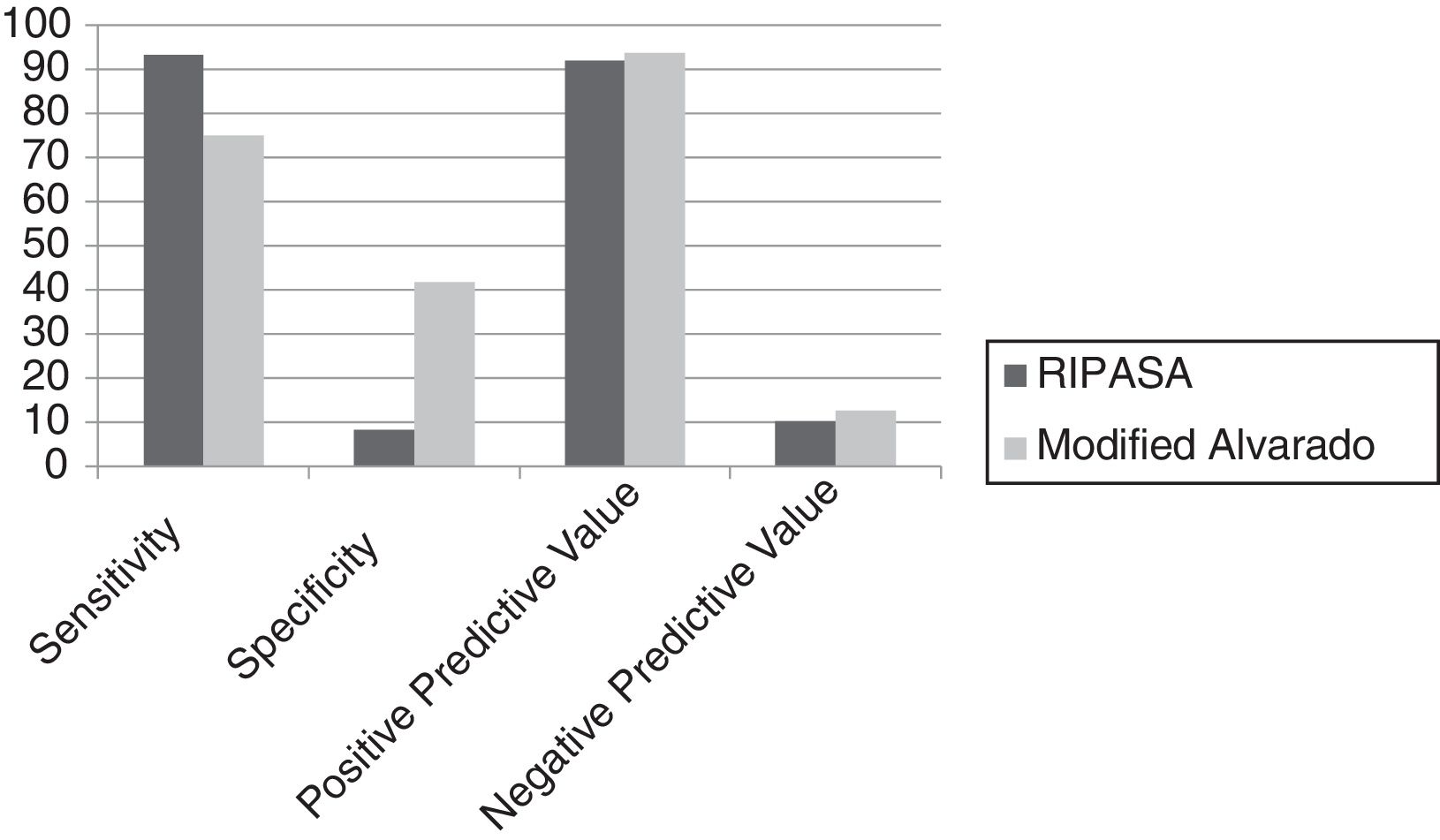
ResultsThe RIPASA score with 8.5 as the optimal cutoff value: ROC curve (area .595), sensitivity (93.3%), specificity (8.3%), PPV (91.8%), NPV (10.1%). Modified Alvarado score with 6 as the optimal cutoff value: ROC curve (area .719), sensitivity (75%), specificity (41.6%), PPV (93.7%), NPV (12.5%).
ConclusionsThe RIPASA score showed no advantages over the modified Alvarado score when applied to patients presenting with suspected acute appendicitis.
La apendicitis aguda es la primera causa de las urgencias quirúrgicas. Permanece como un diagnóstico difícil de establecer, particularmente entre jóvenes, ancianos y mujeres en edad reproductiva, en los cuales una serie de condiciones inflamatorias pueden presentar síntomas y signos similares a los de la apendicitis aguda. Diversos sistemas de puntuación se han creado con el fin de incrementar la certeza diagnóstica; estos son baratos, no invasivos y fáciles de usar o reproducir. La escala de Alvarado modificada es probablemente la más difundida y de mayor aceptación en los servicios de urgencias del mundo. Por otro lado, la escala RIPASA fue elaborada en 2010 con mejor sensibilidad y especificidad. En México se encuentran pocos estudios que comparen los diversos sistemas de puntuación en apendicitis. El objetivo es comparar la escala de Alvarado modificada y la escala RIPASA para el diagnóstico de pacientes con dolor abdominal y sospecha de apendicitis aguda.
Material y métodosSe realizó un estudio observacional, analítico y prolectivo, de julio de 2012 a febrero 2014 en el Hospital Universitario de Puebla. Las encuestas en proceso de evaluación fueron aplicadas a los pacientes con sospecha clínica de apendicitis.
ResultadosEscala de RIPASA: curva ROC/PC 8.5 (área 0.595), sensibilidad (93.3%), especificidad (8.3%), VPP (91.8%), VPN (10.1%). Escala de Alvarado modificada: Curva ROC/PC 6 (área 0.719), sensibilidad (75%), especificidad (41.6%), VPP (93.7%), VPN (12.5%).
ConclusionesLa escala de RIPASA contrastada con la escala de Alvarado modificada no mostró ventajas al aplicarse a pacientes con sospecha de apendicitis aguda.
Acute appendicitis is the first cause of surgical emergencies worldwide, with an incidence of 1.17 to 1.9 per 1,000 inhabitants per year and a lifetime risk of presenting with it of 8.6% in men and 6.7% in women. The most common age range is 25-35 years of age.1,2
Despite its being a common health problem, the diagnosis of acute appendicitis is still difficult to make, especially in young persons, the elderly, and in reproductive-age women. Various genitourinary or gynecologic inflammatory conditions can present with signs and symptoms similar to those of acute appendicitis.3 Diagnosis is based purely on the clinical history and physical examination, combined with the results of laboratory studies, such as a high white cell count.4
Late appendectomy to improve diagnostic accuracy increases the risk for appendicular perforation and sepsis, augmenting morbidity and mortality (surgical site infection 8-15%, perforation 5-40%, abscesses 2-6%, sepsis and death 0.5-5%).1,3 In contrast, premature diagnosis of appendicitis leads to reduced diagnostic accuracy with a consequent rise in negative or unnecessary appendectomies that have been reported at approximately 20-40%.3 Ultrasound and tomography imaging can improve diagnostic accuracy, but are expensive and not always available at healthcare centers.3,5
Different scoring systems have been created to increase the diagnostic accuracy of appendicitis that are low-cost, noninvasive, and easy to use or reproduce.4,5 They assign numerical values to define signs and symptoms. Clinical signs of abdominal pathology (type, pain location and migration, temperature, signs of peritoneal irritation, nausea, and vomiting, among others) and laboratory findings (leukocytosis) are generally used.5
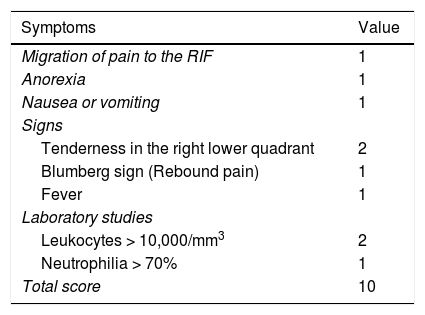
The modified Alvarado score is probably the most widely used and accepted at emergency services, worldwide, with 68-82% sensitivity and 75-87.9% specificity1,5 (Table 1). It classifies patients with abdominal pain in the right iliac fossa into 3 groups of appendicitis probability: a) low risk (0-4 points, 7.7% probability of appendicitis), b) intermediate risk (5-7 points, 57.6% probability of appendicitis) and c) high risk (8-10 points, 90.6% probability of appendicitis).1
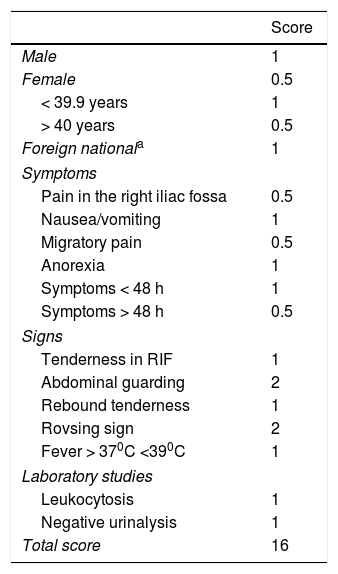
The Raja Isteri Pengiran Anak Saleha appendicitis (RIPASA) scoring system is relatively new. It was developed in 2010 at the RIPAS Hospital of Brunei and has improved sensitivity (98%) and specificity (83%).1,4 Its parameters are described in Table 2. Score interpretation suggests 4 management groups: a) < 5 points (unlikely, patient observation) b) 5-7 points (low probability, emergency room observation, abdominal ultrasound), c) 7.5-11.5 points (high probability, surgical evaluation and preparation for appendectomy), and d) > 12 points (appendicitis diagnosis, appendectomy).1
RIPASA score.
| Score | |
|---|---|
| Male | 1 |
| Female | 0.5 |
| < 39.9 years | 1 |
| > 40 years | 0.5 |
| Foreign nationala | 1 |
| Symptoms | |
| Pain in the right iliac fossa | 0.5 |
| Nausea/vomiting | 1 |
| Migratory pain | 0.5 |
| Anorexia | 1 |
| Symptoms < 48 h | 1 |
| Symptoms > 48 h | 0.5 |
| Signs | |
| Tenderness in RIF | 1 |
| Abdominal guarding | 2 |
| Rebound tenderness | 1 |
| Rovsing sign | 2 |
| Fever > 370C <390C | 1 |
| Laboratory studies | |
| Leukocytosis | 1 |
| Negative urinalysis | 1 |
| Total score | 16 |
RIF: Right iliac fossa.
Few studies comparing the different scoring systems for appendicitis have been conducted in Mexico. A study by Reyes-García at the Hospital General de México had the following results: 89.5% sensitivity and 69.2% specificity with the Alvarado score and 91.2% sensitivity and 84.6% specificity with the RIPASA score.2 Therefore, the aim of the present study was to increase the diagnostic accuracy of appendicitis through a comparison of the modified Alvarado score and the RIPASA score that are used for diagnosing patients with abdominal pain and suspected acute appendicitis.
Materials and methodsAn analytic and observational study was conducted within the time frame of July 2012 and February 2014 at the Hospital Universitario de Puebla.
It included patients with the presumptive diagnosis of acute appendicitis operated on at the Hospital Universitario de Puebla. The study patients met the requisites to be evaluated by the two scores and were of either sex and any age. The scores were applied by general surgery residents, previously instructed in filling them out correctly. Patients that did not have the complete laboratory work-up to be evaluated by the two scores were excluded from the study. Patients that were initially suspected of presenting with acute appendicitis that was ruled out before surgery were eliminated from the study.
The variables analyzed were age, surgical result, and score results from the modified Alvarado score and the RIPASA score.
The data analysis was carried out through descriptive statistics of the demographic data of the population, measures of central tendency, and analyses for diagnostic tests (sensitivity, specificity, and positive and negative predictive values). An ROC curve was then plotted to evaluate both scores using the SPSS version 20.0 software.
ResultsSeventy-two patients operated on for suspected appendicitis within the time frame of February 2013 and February 2014 were evaluated. The two scores were completed before the surgical event. All patients had abdominal x-rays in 2 positions, as part of the study protocol. Twenty-one women had abdominal ultrasound and 17 patients had a non-contrasted abdominal tomography scan. The youngest study patient was 9 years old and the oldest patient was 85 years old. The population was predominantly young, with a mean age of 36.79 ± 20.53 years. The male to female ratio was 1:2.4, with 21 males (29.2%) and 51 females (70.8%).
An initial pilot group was made up of 17 patients (23.6%) that underwent histopathologic study to verify concordance with the postoperative diagnosis dictated by the surgeon upon completing the surgery. All the diagnoses stated by the surgeon were confirmed through histopathologic study.
Of the 72 patients operated on with suspected acute appendicitis, 41 cases (56.9%) corresponded to uncomplicated appendicitis, 19 cases (26.4%) to complicated appendicitis, and 12 cases (16.7%) to a diagnosis different from appendicitis, including lily-white appendix.
The 60 patients with an operative finding of appendicitis had a histopathologic diagnosis corresponding to that pathology.
An independent calculation was performed to evaluate the two scores: ROC curve, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). Both scores were evaluated by a committee of experts that, by consensus, determined 8.5 points as the optimum threshold score for diagnosing appendicitis with the RIPASA score. The results were: ROC curve (area 0.595), sensitivity (93.3%), specificity (8.3%), PPV (91.8%), and NPV (10.1%). The optimum threshold score for the modified Alvarado score for diagnosing appendicitis was 6 points. The results were: ROC curve (area 0.719), sensitivity (75%), specificity (41.6%), PPV (93.7%), and NPV (12.5%) (fig. 1).
Discussion and conclusions
Acute appendicitis diagnosis is made through the clinical history and physical examination of the patient with 75 to 90% accuracy, but it should be supported by laboratory studies.6,7 Complete physical examination of the abdomen should include digital rectal examination and women should undergo a pelvic examination. Incorrect or late diagnosis increases the risk for complications, such as surgical wound infection (8 to 15%), appendiceal perforation (5 to 40%), abscesses (2 to 6%), and sepsis and death (0.5 to 5%).8
The modified Alvarado score and the RIPASA score can easily be applied by medical residents on medical-surgical emergency service rotation, as was the case at our hospital for the present study.9–11
One out of every 15 or 20 Mexicans will present will acute appendicitis at some point in their lives. Clinical manifestations in the prodromal phase can be vague and uncertain and similar to those of other pathologies. Failure to make early diagnosis increases the risk for complications. In the present study, a greater number of patients presented with uncomplicated appendicitis, denoting adequate time of operation. Delayed diagnosis also increases hospital costs.2,6,12
The Alvarado score can be used as a triage method in patients with suspected acute appendicitis. Our study results demonstrated higher specificity with the modified Alvarado score than with the RIPASA score, contrary to what is reported in the literature.1,7,13–15 The RIPASA proposed in 2010 evaluates other parameters, such as age and disease progression time, but those data had no statistical significance in our study.1,2
In conclusion, the RIPASA score demonstrated no advantage over the modified Alvarado score. The modified Alvarado score is currently the most widely used at emergency services. The RIPASA score has shown greater diagnostic accuracy in different studies, but no statistically significant data were found in the present study to support its routine application.
In our study, the RIPASA score had high sensitivity and low specificity because it already has positive scores for our population, such as the “foreign national” item and 6 points for physical examination, depending on who performs it. Our patients did not have an abdominal tomography scan, which is the criterion standard for appendicitis diagnosis. Another factor could be that the RIPASA score is not validated for the Spanish language. We consider that it was developed for a different population from ours, and as Anand Singla stated in his conclusions, results of the RIPASA score should be evaluated in studies with a larger number of patients from different geographic regions that includes both sexes.16
Ethical disclosuresProtection of human and animal subjectsThe authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of dataThe authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consentThe authors have obtained the written informed consent of the patients or subjects mentioned in the article. The corresponding author is in possession of this document.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Díaz-Barrientos CZ, Aquino-González A, Heredia-Montaño M, Navarro-Tovar F, Pineda-Espinosa MA, Espinosa de Santillana IA. Escala RIPASA para el diagnóstico de apendicitis aguda: comparación con la escala de Alvarado modificada. Revista de Gastroenterología de México. 2018;83:112–116.

