
Cysts of the spleen are an unusual pathology in daily clinical and surgical practice, with fewer than 1,000 cases reported in the literature. The majority of patients are asymptomatic, and diagnosis is usually based on imaging techniques. Surgical indication and treatment are a challenge for surgeons. We present herein the case of a patient with a primary cyst of the spleen as an infrequent cause of dyspepsia.
A 21-year-old woman with an unremarkable past history presented with clinical symptoms of early satiety, postprandial fullness, left epigastrium-hypochondrium pain upon eating, and a 3-kg weight loss. Physical examination revealed pain upon deep palpation of the left hemiabdomen. Abdominal ultrasound identified a 7-cm splenic lesion that was isoechoic, with little acoustic enhancement, and well-defined contours. Hemogram and biochemical tests were unaltered, hemagglutination-hydatidosis was negative, and the Ca 19.9 and carcinoembryonic antigen (CEA) markers were normal. The evaluation was completed through CT that showed an oval-shaped lesion with well-defined contours in the spleen. Its diameters measured 80 x 72 x 68mm and there were no internal enhancements or solid poles. The stomach was displaced, but there were no signs suggestive of malignancy. Primary cyst of the spleen was suspected, and laparoscopic fenestration was performed with no complications. The intraoperative cytology results were acellular serous diathesis and the histology study reported simple, flat epithelial lining that was positive for pankeratin (AE1-AE3) and calretinin and negative for CEA and Ca 19.9 (fig. 1A-D).
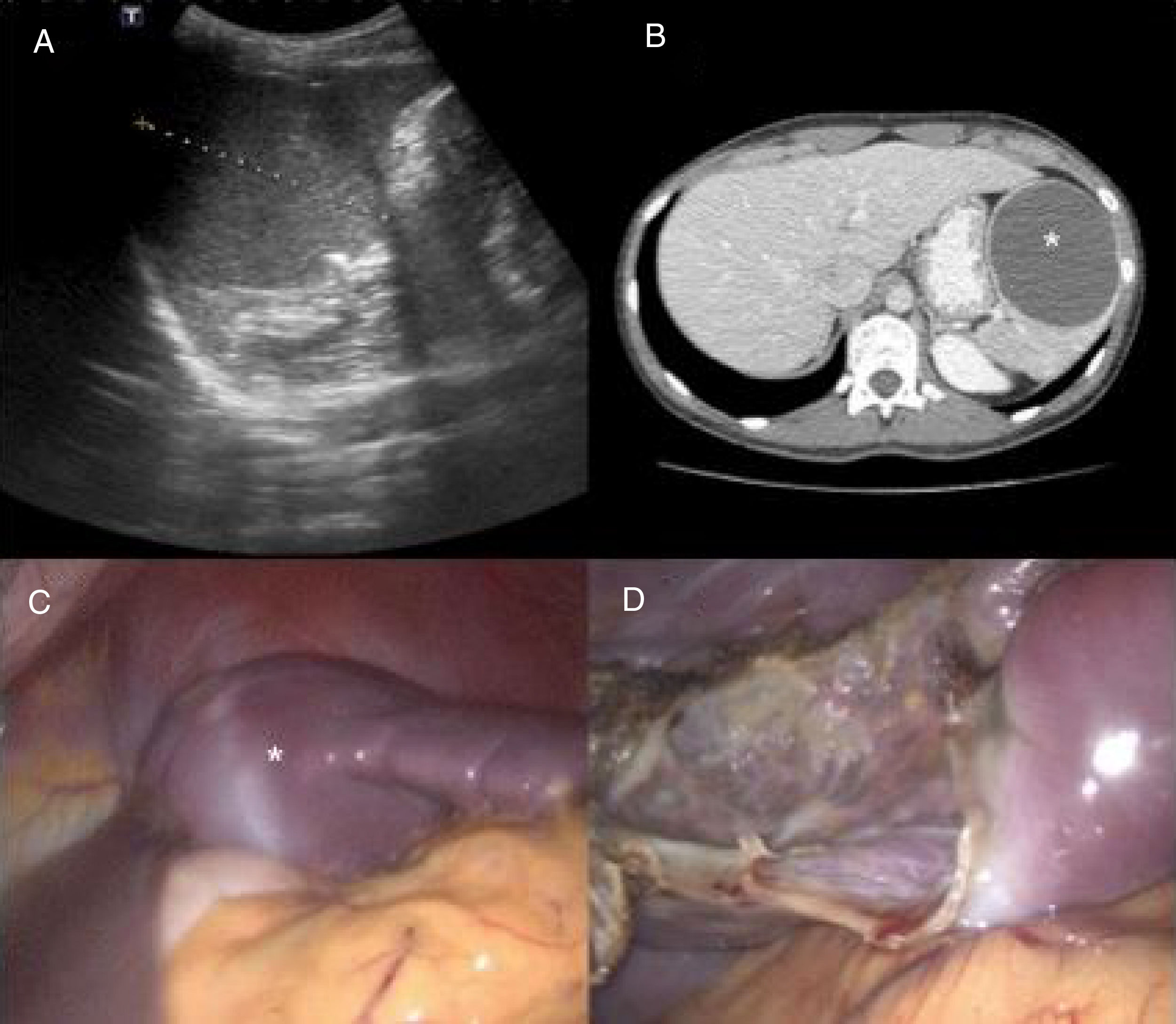
 Preoperative abdominal ultrasound: splenic lesion measuring 7cm in diameter with little acoustic enhancement and well-defined contours. B) Preoperative computed tomography scan: well-defined oval-shaped lesion consistent with a cyst of the spleen (asterisk). Note the displacement of the stomach. C) Laparoscopic intraoperative image: splenic cyst (asterisk) compressing the stomach before fenestration. D) Laparoscopic intraoperative image: remnant of the splenic parenchyma after fenestration.")
A) Preoperative abdominal ultrasound: splenic lesion measuring 7cm in diameter with little acoustic enhancement and well-defined contours. B) Preoperative computed tomography scan: well-defined oval-shaped lesion consistent with a cyst of the spleen (asterisk). Note the displacement of the stomach. C) Laparoscopic intraoperative image: splenic cyst (asterisk) compressing the stomach before fenestration. D) Laparoscopic intraoperative image: remnant of the splenic parenchyma after fenestration.
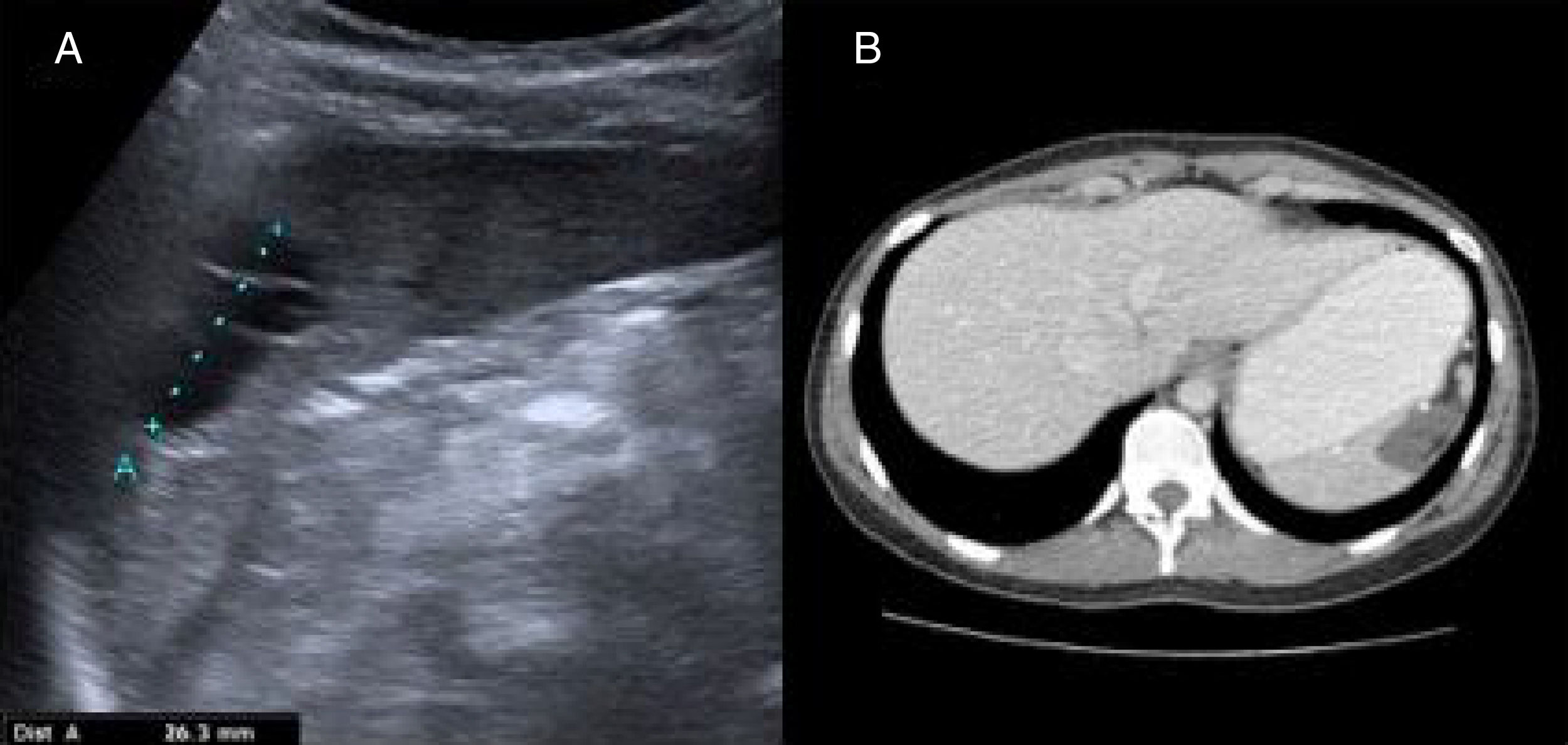
The symptoms of the patient improved and she gained 6kg that she has maintained throughout her progression. The ultrasound study at 6 months after the intervention and the CT scan at one year showed a small cystic remnant and postoperative changes that did not affect the neighboring structures. The size of the remnant did not increase between the time the 2 imaging studies were carried out (fig. 2 A and B).
 Postoperative abdominal ultrasound: a well-defined, anechoic, polylobulated lesion with echogenic internal septa in the interpolar region of the spleen, measuring 32mm in diameter, consistent with a cystic remnant. B) Computed tomography scan: altered splenic contour with a 22 x 23mm uniform hypodense lesion consistent with a postoperative cystic remnant.")
A) Postoperative abdominal ultrasound: a well-defined, anechoic, polylobulated lesion with echogenic internal septa in the interpolar region of the spleen, measuring 32mm in diameter, consistent with a cystic remnant. B) Computed tomography scan: altered splenic contour with a 22 x 23mm uniform hypodense lesion consistent with a postoperative cystic remnant.
Cysts of the spleen are rare. The Mediterranean countries are endemic zones1 where the Echinococcus granulosus parasites predominate. Noninfectious cysts include the primary cysts, which are characterized by the epithelial lining, and the secondary cysts (pseudocysts), which are more frequent and generally have a posttraumatic origin.
Primary cyst incidence is only 0.07%2 and they are predominant in young women. They are usually incidental findings but can cause clinical symptoms due to adjacent organ compression, as occurred in our patient through gastric compression.
The etiopathogenesis of this disease is unknown. There are several types of epithelial lining: positivity for CEA and Ca 19.9 in epithelial cysts and positivity for pankeratin (AE1-AE3) and calretinin in mesothelial cysts stand out.3
The dilemma is when and how to treat them. Treatment is accepted for symptomatic cysts and those> 5cm, due to the risk for complications, such as rupture, bleeding, and infection.
There are high rates of recurrence and complications with percutaneous treatment (aspiration and treatment with alcohol),4 and it is reserved for inoperable patients. Surgical techniques include total or partial splenectomy, decapsulation (complete membrane extirpation) and fenestration (resection that puts the cavity of the cyst in contact with the peritoneum)5 and all can be performed laparoscopically. The current trend is toward spleen-sparing techniques to prevent immunosuppression and thrombocytosis.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Elosua González A, Nantes Castillejo O, Tarifa Castilla A, Llanos Chávarri MC. Quiste mesotelial primario esplénico como causa infrecuente de dispepsia: a propósito de un caso. Revista de Gastroenterología de México. 2018;83:463–465.

