
At the Upper Gastrointestinal Tract Clinic of the Hospital General de Mexico, achalasia treatment has been standarized through strictly graduated cardiomyotomy. This procedure guarantees a complete myotomy for the satisfactory resolution of dysphagia, a characteristic symptom of achalasia. To ensure the inclusion of the entire lower esophageal sphincter, an 8cm Penrose drain is placed at the surgical site 6cm above the gastroesophageal junction and 2cm in a caudal direction, for accurate laparoscopic measuring. The aim of our study was to evaluate the results of this technique.
Materials and methodsA descriptive, retrospective, longitudinal, and observational study was conducted on a cohort of patients diagnosed with achalasia at the Upper Gastrointestinal Tract Clinic of the Hospital General de México “Dr. Eduardo Liceaga”.
ResultsThe study included 48 patients, 40 of whom had no prior surgical treatment and 8 that presented with recurrence. Forty-seven patients (97.9%) underwent a laparoscopic procedure and conversion to open surgery was required in 2 of them (4.25% conversion rate). Postoperative progression was satisfactory in all cases, with mean oral diet commencement at 52h and mean hospital stay of 5.7 days. No recurrence was registered during the mean follow-up period of 35.75 months and there were no deaths.
ConclusionsLaparoscopic graduated (strictly measured) cardiomyotomy with anterior fundoplication is a reproducible, efficacious, and safe option for the surgical treatment of achalasia.
En la Clínica de Tracto Digestivo Superior del Hospital General de México, el tratamiento de la acalasia se ha estandarizado mediante la realización de una cardiomiotomía estrictamente graduada que permite garantizar una miotomía completa para resolver de forma satisfactoria la disfagia característica de esta enfermedad. Un penrose de 8cm, se coloca sobre el lecho quirúrgico, para garantizar la inclusión de todo el EEI, 6cm por arriba de la UGE y 2cm en sentido caudal, para asegurar la medición laparoscópica. El objetivo del estudio fue evaluar los resultados obtenidos con esta técnica.
Material y métodosEstudio descriptivo, retrospectivo, longitudinal, observacional, en una cohorte de pacientes con diagnóstico de acalasia, en la Clínica de Tracto Digestivo Superior, del Hospital General de México «Dr. Eduardo Liceaga».
ResultadosSe incluyeron 48 pacientes; 40 sin tratamiento quirúrgico previo y 8 con recurrencia. En 47 casos el abordaje fue laparoscópico (97.9%); se requirió conversión a procedimiento abierto en 2 casos (tasa conversión 4.25%). La evolución postoperatoria fue satisfactoria en todos los casos, con inicio de la vía oral a las 52h en promedio y una estancia intrahospitalaria promedio de 5.7 días. Durante el seguimiento de 35.75 meses en promedio no se han registrado recurrencias. No se presentó mortalidad.
ConclusionesLa cardiomiotomía graduada (estrictamente medida) con funduplicatura anterior mediante abordaje laparoscópico es una opción reproducible, eficaz y segura para el tratamiento quirúrgico de la acalasia.
Achalasia is a primary motor disorder of the esophagus that is characterized by the absence of esophageal peristalsis and alteration in the lower esophageal sphincter (LES) relaxation in response to swallowing,1 hindering esophageal emptying and causing gradual proximal esophageal dilation.2 It was first described in 1674 by Thomas Willis who treated the disease by freeing the obstruction with a whale bone, and it was not until 1913 that Hurst coined the term achalasia.3,4
This motility disorder is caused by loss of the inhibitory activity and degeneration of the ganglion cells in the myenteric plexus.5 The destruction of the inhibitory neurons that produce nitric oxide and vasoactive intestinal peptide is most likely the result of an inflammatory process, whose triggering mechanism is still unknown.6 Achalasia incidence is less than 1 in 100,000 inhabitants per year and its prevalence is 10 in 100,000, with no preference for race or sex. It mainly affects the 30 to 60-year-old age group.7,8
Clinical presentation is characterized by progressive dysphagia, thoracic pain, and the regurgitation of partially digested food, having an important secondary impact on the nutritional status of the patients.9 High-resolution manometry is the criterion standard for making the diagnosis and categorizing the patients into 3 subtypes to establish and predict response to surgical treatment.10 Esophagram and endoscopy are complementary studies for this pathology.8
Achalasia treatment can be medical, endoscopic, or surgical.8 Currently, the treatment of choice is the modified Heller cardiomyotomy, associated with an antireflux procedure. At the esophageal clinic of the Hospital General de México, treatment has been standardized through laparoscopic graduated (strictly measured) cardiomyotomy with the Dor anterior fundoplication. There are no Mexican studies describing the efficacy of this surgical technique or its results.
The aim of the present study was to describe the experience at an advanced specialty clinic in the diagnosis and treatment of patients with achalasia, through a laparoscopic graduated cardiomyotomy technique with anterior fundoplication. This graduated technique ensures the performance of a complete myotomy with an acceptable minimum length.
Materials and methodsA retrospective, descriptive, longitudinal, observational study was conducted on a cohort of patients diagnosed with achalasia at the Upper Gastrointestinal Tract Clinic of the General Surgery service at the Hospital General de México, “Dr. Eduardo Liceaga”. Patients of both sexes diagnosed with achalasia that underwent surgical treatment within the time frame of January 1, 2010, and June 30, 2014 were included in the study. They were over 18 years of age and had complete medical histories.
All the procedures were performed by the same surgical group of 2 surgeons and residents, with the same steps in each procedure, and follow-up was carried out by the same surgical group.
Treatment at the Upper Gastrointestinal Tract Clinic of the Hospital General de México has been standardized over the last few years through a strictly graduated cardiomyotomy that ensures complete myotomy and satisfactorily resolves the dysphagia that is characteristic of achalasia. An 8-cm Penrose drain is placed at the surgical site, to make sure the entire LES is included, 6cm above the gastroesophageal junction (GEJ) and 2cm in the caudal direction, ensuring correct measurement in the laparoscopy.
The following steps of the standardized technique were used in all the cases:
Pneumoperitoneum with OptiView with 5 trocars
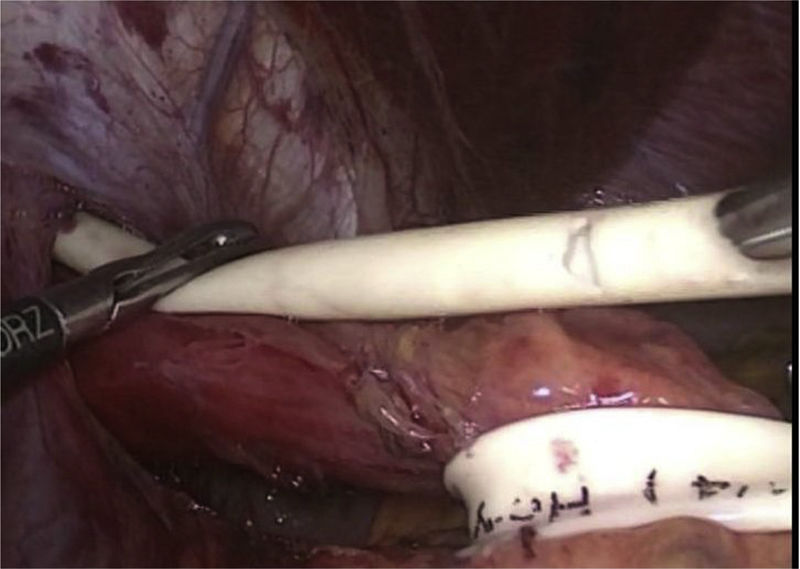
Dissection of the hiatus identifying the vagal nerves and esophageal traction with the Penrose drain. The intrathoracic esophagus is freed, until achieving a distance of more than 8cm from the GEJ, measured with the Penrose drain (fig. 1).

Myotomy is performed on the distal esophagus in a caudal direction up to the previously identified distance and myotomy is then performed on the stomach in the same direction up to the previously measured distance.
Endoscopy is carried out to corroborate the location of the GEJ and the methylene blue test is done to identify possible perforation.
The short vessels are freed and the Dor fundoplication is performed with 5 sutures on each side of the myotomy.
The variables analyzed were divided into general demographics, preoperative variables, intraoperative variables, immediate postoperative variables, and follow-up variables. Descriptive and inferential statistics were carried out with the IBM SPSS version 22 software. Informed consent to undergo all procedures was obtained from the patients.
ResultsA total of 54 patients were identified, 48 of which were included in the study, given that the medical records were incomplete in 6 cases.
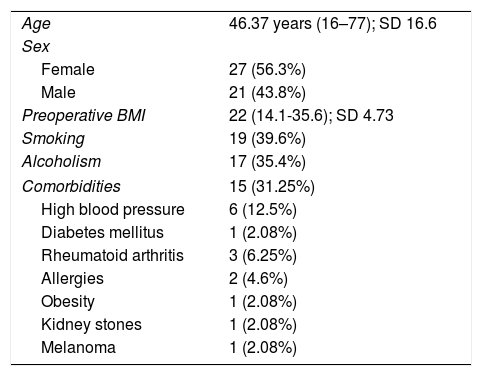
Table 1 shows the demographic variables.
Demographic variables.
| Age | 46.37 years (16–77); SD 16.6 |
| Sex | |
| Female | 27 (56.3%) |
| Male | 21 (43.8%) |
| Preoperative BMI | 22 (14.1-35.6); SD 4.73 |
| Smoking | 19 (39.6%) |
| Alcoholism | 17 (35.4%) |
| Comorbidities | 15 (31.25%) |
| High blood pressure | 6 (12.5%) |
| Diabetes mellitus | 1 (2.08%) |
| Rheumatoid arthritis | 3 (6.25%) |
| Allergies | 2 (4.6%) |
| Obesity | 1 (2.08%) |
| Kidney stones | 1 (2.08%) |
| Melanoma | 1 (2.08%) |
BMI: body mass index; SD: standard deviation
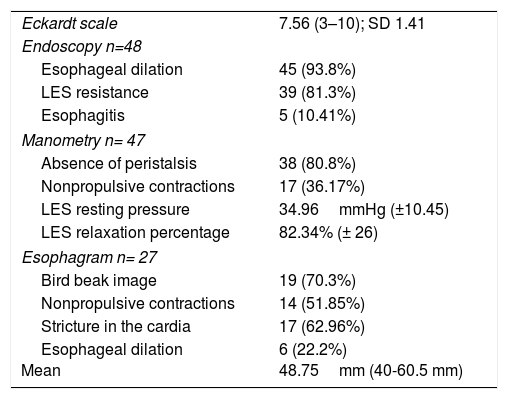
In the referred patients diagnosed with achalasia, the study protocol included endoscopy, manometry, and esophagram. Only 2 cases had high-resolution manometry, reported as Chicago I and III. Table 2 shows the clinical characteristics and the preoperative laboratory work-up.
Preoperative characteristics.
| Eckardt scale | 7.56 (3–10); SD 1.41 |
| Endoscopy n=48 | |
| Esophageal dilation | 45 (93.8%) |
| LES resistance | 39 (81.3%) |
| Esophagitis | 5 (10.41%) |
| Manometry n= 47 | |
| Absence of peristalsis | 38 (80.8%) |
| Nonpropulsive contractions | 17 (36.17%) |
| LES resting pressure | 34.96mmHg (±10.45) |
| LES relaxation percentage | 82.34% (± 26) |
| Esophagram n= 27 | |
| Bird beak image | 19 (70.3%) |
| Nonpropulsive contractions | 14 (51.85%) |
| Stricture in the cardia | 17 (62.96%) |
| Esophageal dilation Mean | 6 (22.2%) 48.75mm (40-60.5 mm) |
LES: lower esophageal sphincter; mm: millimeters; mmHg: millimeters of mercury; SD: standard deviation
Eight cases (16.7%) had previous medical treatment, registered as follows: one case (2.08%) had Savary dilation, 6 (12.5%) had pneumatic dilation, and one (2.08%) had pharmacotherapy (calcium channel blockers). None of those cases responded adequately to the previous medical treatment and therefore were programmed for surgery at the esophageal clinic.
Eight cases presented with recurrence, 5 of which had received treatment at the Hospital General de México, but not at the esophageal clinic, and 3 were operated on at another hospital. A new myotomy with anterior fundoplication was required in 7 (87.5%) cases, because the first procedure was incomplete. Firm fibrosis in the GEJ was found in one case during the reintervention and only the previous fundoplication was dismantled, the fibrosis was freed, and anterior re-fundoplication was carried out, with no need to widen or complete the myotomy.
Graduated cardiomyotomy with an 8-cm long Penrose drain as described above was performed on the 48 patients (100%). In all the cases, the Dor fundoplication was performed as the antireflux procedure. Myotomy was not smaller than 8cm in total in any of the cases.
The approach was laparoscopic in 47 of the cases (97.9%) and the open approach was opted for in one case (2.09%), because the patient had a history of multiple laparotomies due to abdominal trauma. Two cases required conversion to open procedures (4.25% conversion rate), due to firm adhesions that prevented safe dissection in both cases. Gastric perforation was detected in one of those cases.
Mean surgery duration was 183min (range: 120-315min, SD 49.89) and mean blood loss was 56ml (range: 5-250ml, SD 44). No transfusions were required in any of the cases.
Intraoperative endoscopy was carried out in 33 cases (68.8%), with adequate passage of the endoscope and no resistance through the GEJ. There was no need to widen the myotomy in any (100%) of the cases. Esophageal perforation was corroborated in 6 cases (12.5%) and gastric perforation in one case (2.1%), after which primary closure was performed.
Intraoperative complications included 2 gastric perforations (4.16%) and 8 esophageal perforations (16.66%), all of which were resolved with intraoperative primary closure. One pneumothorax associated with esophageal dissection (2.08%) required the placement of an intrapleural catheter during the intraoperative period. There were no complications in the other 37 cases (77.08%).
Postoperative progression was satisfactory in all the cases, with no need for reintervention in any of them. Oral diet was begun at a mean 52h (range: 6 to 192h) and mean hospital stay was 5.7 days (range: 2-27 days). Prolonged stay was associated with the cases of esophageal or gastric perforation, due to initial delay of the oral diet of 72 to 120 postoperative hours. No infectious complications were registered. All patients were released due to improvement and no deaths were registered in our case series.
Part of the follow-up at the esophageal clinic is the evaluation of patients 7 days after the procedure, at postoperative month one, three, and six, and then every year. Mean follow-up was 35.76 months.
Symptom evaluation is routinely carried out using the Eckardt scale and the results of which at 6 postoperative months were: 29 patients (60.4%) with 0 points, 10 patients (20.8%) with 1 point, and 3 patients (6.3%) with 2 points. The preoperative and postoperative results were compared using the t test for related samples, and they were statistically significant (p < 0.001).
Discussion and conclusionsSince the 1990s, the minimally invasive approach has been the criterion standard for treating achalasia, because it is a safe, effective, and reproducible technique.11–14 The type of fundoplication that should be performed in those patients as an antireflux procedure is currently a subject of much debate. Over time, numerous techniques have been developed (Nissen, Toupet, Dor, posterior esophagogastropexy), providing multiple therapeutic options.15,16 An important guide for choosing the type of fundoplication is postoperative dysphagia, which involves the total technique as opposed to the partial ones (15 vs 2.8% p=0.001).17,18 Likewise, not performing an antireflux procedure has been proposed, given that low asymptomatic GERD rates have been demonstrated in follow-up at 5 years in 75% of patients, with antireflux medically corrected in the remaining percentage.19
Up to now, the large case series published on cardiomyotomy for achalasia patients20,21 show that anterior partial fundoplication has outstanding results as an antireflux method, with up to 60 months of follow-up. Numerous studies have compared posterior partial fundoplication with anterior partial fundoplication and both techniques have similar results in relation to reflux control and dysphagia symptoms. However, better esophageal emptying has been observed with the anterior partial technique.22–24 Fundoplication is imperative in the integrated treatment of achalasia to offer better quality of life to the patients and reduce morbidity from GERD manifestations. Nevertheless, more studies comparing the two techniques are required.
Over time, the length of the myotomy has been established to be at least 6cm, 4 proximal and 2 distal, to ensure that all LES fibers are included.25 We consider adequate measuring of the myotomy for laparoscopy essential for reducing recurrence in those patients, because the main failure in this technique is incomplete myotomy, in addition to the fact that the proportions of length can be lost with laparoscopy.26
Timed barium esophagram is useful in evaluating recurrence symptoms and when surgical reintervention is required in patients with long progression of the disease. Patients that present with stasis ≥ 5cm during the study are at 8-fold greater risk for reintervention, without a direct association with increased LES pressure.27 This method is an accessible manner for carrying out patient follow-up and determining outcome.
No recurrence was detected in our group of patients operated on with this technique. The present study is the first to be conducted in Mexico to evaluate graduated cardiomyotomy that is strictly measured, performed with Dor anterior fundoplication.
In conclusion, laparoscopic graduated (strictly measured) cardiomyotomy with anterior fundoplication is an efficacious, reproducible, and safe option for the surgical treatment of achalasia, according to our study results.
Graduated cardiomyotomy offers satisfactory results with no sign of recurrence or postoperative dysphagia, in accordance with the Eckardt scale applied to the patients, adequately achieving the surgical objective.
We consider the Dor anterior fundoplication the antireflux procedure of choice for those patients, because it protects the dissection area and reduces the dysphagia associated with fundoplication.
At present, no disease recurrence has been registered at the clinic of our hospital in patients that underwent this technique.
No patient has required treatment after the surgical procedure.
Postoperative follow-up through the Eckardt scale and timed barium esophagram is an adequate option for establishing outcome and the need for reintervention in those patients.
Ethical responsibilitiesProtection of persons and animalsThe authors declare that no experiments were performed on humans or animals for this study.
Data confidentialityThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
The authors wish to thank the entire medical and administrative personnel at the Upper Gastrointestinal Tract Clinic of the Hospital General de México “Dr. Eduardo Liceaga”.
Please cite this article as: Etchegaray-Dondé A, Rodríguez-Espínola G, Higuera-Hidalgo F, Ortiz-Higareda V, Chapa-Azuela O, Etchegaray-Solana A. Cardiomiotomía graduada con funduplicatura anterior laparoscópica en acalasia, experiencia de 48 casos. Revista de Gastroenterología de México. 2018;83:106–111.

