

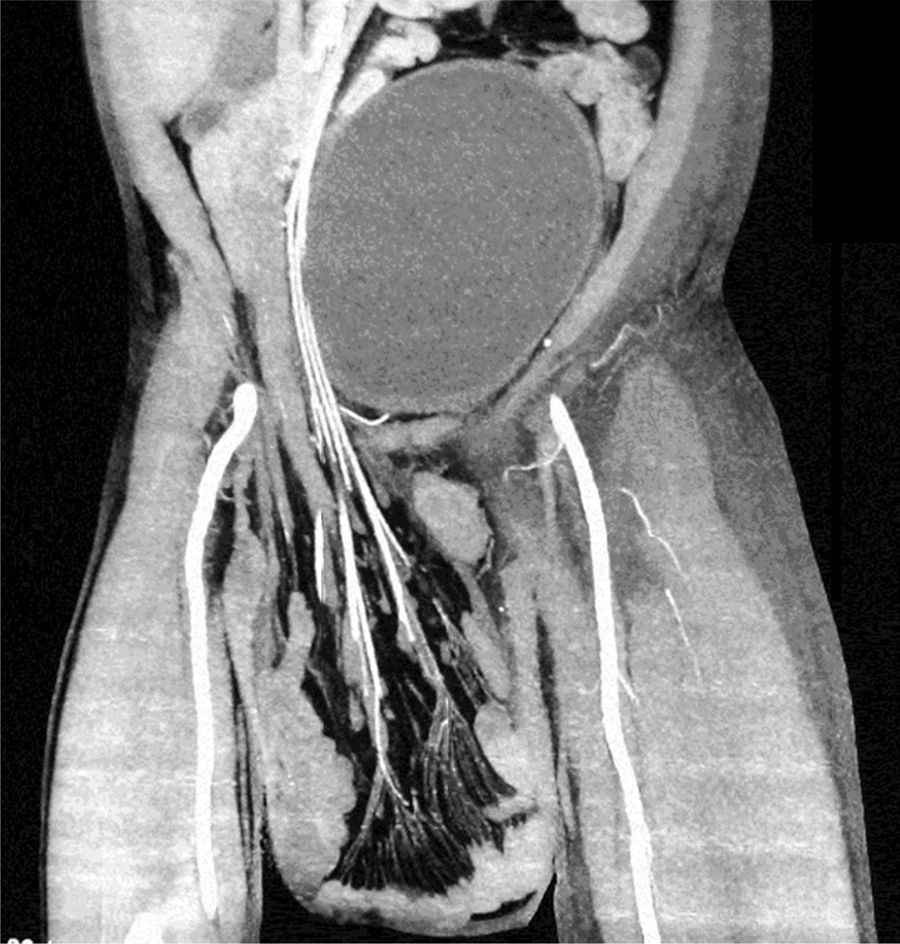



A 55-year-old man with a 30-year history of giant inguinoscrotal hernia (fig. 1) came to the emergency department due to urinary obstruction. A Foley catheter was placed and an abdominal angiotomography scan was carried out that revealed the small bowel within a right inguinoscrotal hernial sac with no vascular involvement (figs. 2 and 3). Laboratory test values were normal. The patient was admitted to the hospital and a Tenckhoff catheter was placed by means of a Veress needle in the left abdominal upper quadrant (fig. 4). The abdominal cavity was insufflated with 800 to 1,000 cc of environmental air. The intra-abdominal pressure was monitored through the Foley catheter connected to an electric pressure transducer. The maximum intra-abdominal pressure gradually reached was 20 cmH20, corresponding to 27.9mmHg. On the tenth day of hospitalization, surgery was carried out to place the bowel in the abdominal cavity and resect the hernial sac. The abdominal wall was strengthened with composite mesh. There were no postoperative complications (fig. 5). This type of surgery is the treatment model that can be offered to patients with giant inguinoscrotal hernia,1–3 enabling satisfactory quality of life.





The authors declare that the procedures followed conformed to the ethical standards of the responsible committee on human experimentation and were in accordance with the World Medical Association and the Declaration of Helsinki.
Data confidentialityThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study.
Conflict of interestThe authors declare that there is no conflict of interest.

