
Tuberculosis is a worldwide public health problem. Despite the advances made in relation to diagnosis, prevention, and treatment, this disease causes millions of deaths annually throughout the world. Known as “the great mimicker”, tuberculosis simulates a large number of diseases and its peritoneal variant can clinically behave like a different abdominal pathology.1–4 Peritoneal tuberculosis occurs in 1 to 3% of the cases of tuberculosis and is the sixth most frequent cause of its extra-pulmonary forms.5 The majority of cases are secondary to a primary pulmonary infection spread by means of the lymphatic system or bloodstream or by intestinal tuberculous lesion contiguity. It can present in 3 forms: a) humid, presenting with free ascites; b) fibrocaseous, as a consequence of the humid state, with the formation of tumors due to lax adhesions of intestinal segments; and c) fibroadhesive or dry, in which there are abdominal masses composed of mesenterium and thickened peritoneum. If not considered among the diagnostic possibilities, it can eventually develop into a complication, such as intestinal obstruction, perforation, abscesses, fistulas, or gastrointestinal bleeding, among others, requiring surgical intervention and having a significant repercussion on morbidity and mortality rates.5,6
A 25-year-old indigenous man, with marked protein-calorie malnutrition, presented with symptoms 20 days prior to his hospital admission of insidious, colicky abdominal pain of moderate intensity, located in the right iliac fossa and accompanied by a measured body temperature of 40°C. He was admitted with the diagnosis of inflammatory acute abdomen: appendiceal adhesions. The patient had a past history of smoking 3-4 cigarettes daily, along with daily drunkenness. Physical examination revealed a body temperature of 39°C, dyspnea with a respiratory rate of 26 breaths per minute, and a flat abdomen, painful upon palpation in the 4 quadrants with signs of peritoneal irritation. The paraclinical tests reported leukocytosis with neutrophilia, moderate anemia, and thrombocytosis. Chest x-ray identified a small right pleural effusion. Exploratory abdominal surgery was performed due to suspicion of appendiceal adhesions and resulted in the following surgical findings: 100ml of free secretion in the cavity and multiple firm adhesions and granulomatous lesions along the small bowel, colon, mesocolon, and omentum. The omentum and cecal appendix were resected (fig. 1A) and processed for their histopathologic study, which reported: chronic granulomatous inflammation with well developed granulomas with a tendency toward confluence and caseous necrosis in both the mesocolon and the omentum, along with acute appendicitis with chronic granulomatous inflammation in the mesoappendix (fig. 1B and 1C). The sent samples were stained with the Ziehl-Neelsen and Grocott special stains, which showed no microorganisms (fig. 1D). Given the histopathology study results, anti-tuberculosis treatment was begun and the response was unsatisfactory. After 6 post-operative days, the patient presented again with abdominal pain and distension and was diagnosed with surgically perforated acute abdomen due to perforation of the small segment. The affected segment was resected and ileostomy was established. However, the patient's condition deteriorated rapidly and after a 30-day progression he died due to septic shock complicated by acute renal insufficiency, acid-base and hydroelectrolytic imbalance, and severe anemia. Autopsy was not performed.
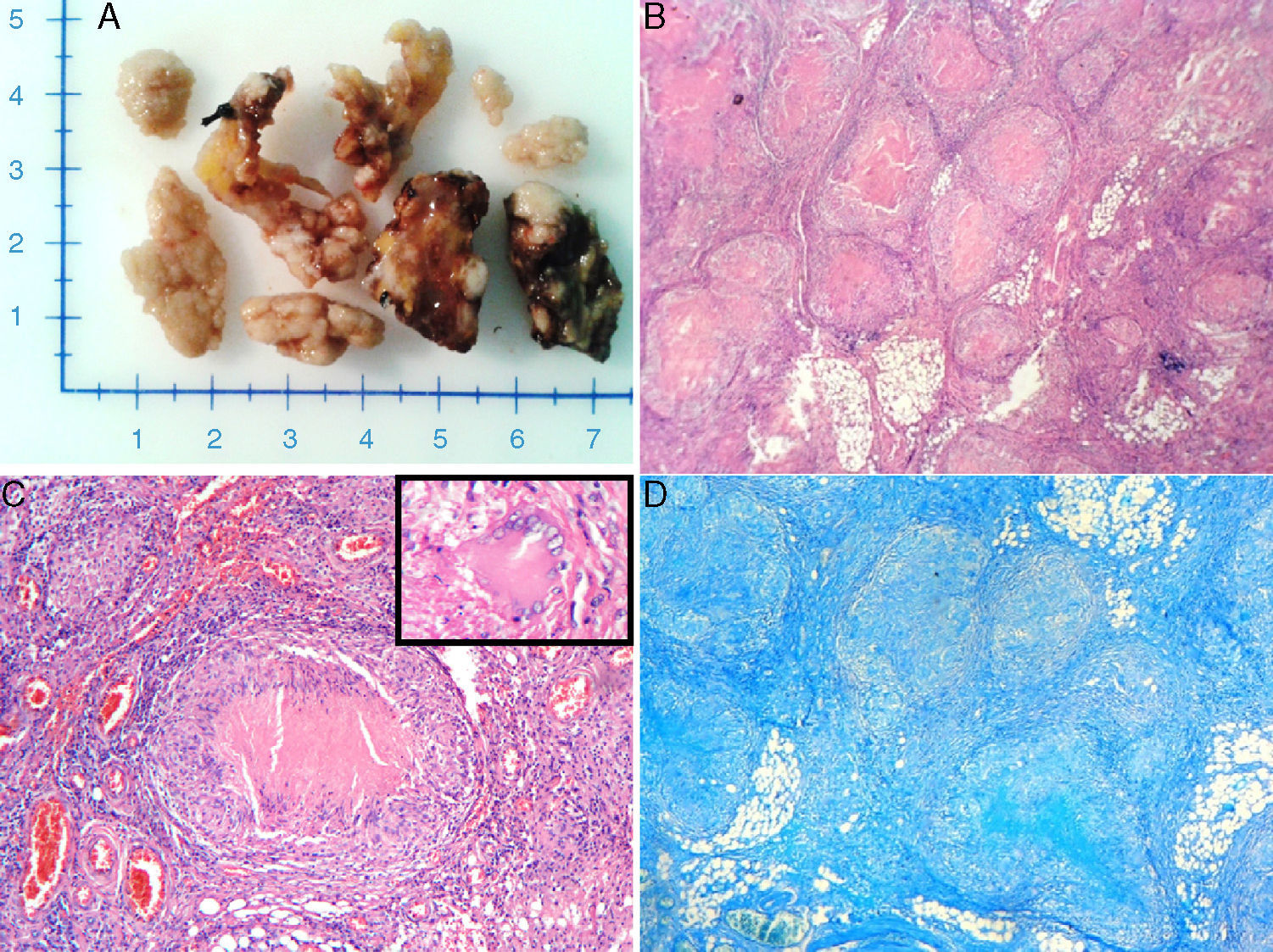
 Macroscopic aspects of fragments of omentum with multiple lesions on raised whitish nodules. B) Panoramic view of the peritoneal tissue, the presence of numerous granulomas with a center of caseous necrosis and epithelioid histiocytes at the periphery. Hematoxylin and eosin stain (x100). C) Granuloma (at the center) formed by epithelioid histiocytes arranged in a palisade, central caseous necrosis, with lymphocytes at the periphery. A Langhans giant cell is also observed (box). Hematoxylin and eosin stain (x400). D) Ziehl-Neelsen stain. Absence of acid-alcohol-resistant bacilli.")
A) Macroscopic aspects of fragments of omentum with multiple lesions on raised whitish nodules. B) Panoramic view of the peritoneal tissue, the presence of numerous granulomas with a center of caseous necrosis and epithelioid histiocytes at the periphery. Hematoxylin and eosin stain (x100). C) Granuloma (at the center) formed by epithelioid histiocytes arranged in a palisade, central caseous necrosis, with lymphocytes at the periphery. A Langhans giant cell is also observed (box). Hematoxylin and eosin stain (x400). D) Ziehl-Neelsen stain. Absence of acid-alcohol-resistant bacilli.
Peritoneal tuberculosis is rare and is a diagnostic challenge.4,5 It is generally secondary to dissemination due to tuberculous lesion contiguity at the level of the intestine. The majority of cases develop in young adults and in women with a 2:1 ratio.4 Clinically, the disease is insidious, developing gradually over weeks to months, with nonspecific symptoms or with few constitutional symptoms, despite the extensive involvement of the peritoneum. The most important symptoms are ascites, abdominal pain, weight loss, and fever,4,7 as was the case with our patient. In the majority of cases, diagnosis is suspected or made during laparoscopy or exploratory laparotomy indicated for other reasons.5,6 Mukhopadhyay et al.6 described 70 cases of abdominal tuberculosis, 7 of which (10%) developed acute appendicitis, similar to that of our patient. Those authors stated that the development of acute abdomen in patients with abdominal tuberculosis is one of the circumstances that enables the eventual etiologic diagnosis of the clinical symptoms of abdominal tuberculosis. To the best of our knowledge, very few cases have been reported with the clinical symptoms of inflammatory acute abdomen similar to those of the present case.6–11 Numerous risk factors for its development have been described, such as human immunodeficiency virus, cirrhosis of the liver, peritoneal dialysis, alcoholism, diabetes, systemic corticoid use, and malnutrition.12 Our patient had an accentuated alcoholic habit and malnutrition. On the other hand, only one sixth of patients are associated with active pulmonary tuberculosis.12 Thus, the absence of radiologic findings does not rule out possible extra-pulmonary infection. The typical macroscopic datum is the presence of whitish nodules of approximately 5mm in diameter dispersed over the peritoneum and viscera,4 as those observed during the exploratory laparotomy of our patient. The classic histopathologic findings are the chronic granulomatous inflammatory reaction made up of activated epithelioid macrophages surrounded by a collar of lymphocytes, plasma cells, and varying degrees of fibrosis, the presence of Langhans multinucleated giant cells, and central caseous necrosis. Special stains, such as the Ziehl-Neelsen stain, can identify the presence of the tuberculous bacillus, but this finding is rare.4 Nevertheless, its absence does not rule it out, due to numerous factors, such as the concentration of the microorganism, the degree of tissue fibrosis, and the patient's immune system. Finally, the fatal progression of our patient could be linked to his poor general state of health (protein-calorie malnutrition), the accentuated alcoholic habit, and the extensive peritoneal involvement (diffuse fibroadhesive tuberculosis) complicated with acute appendicitis and the formation of appendiceal adhesions, and the later postoperative complication of bowel segment perforation followed by septic shock resulting in death. In regard to this, a study of 209 patients with abdominal tuberculosis reported that 17% (35 patients) required surgical intervention, of which 22% (8 cases) died in the postoperative period.7 It can therefore be considered that the necessity of surgical intervention in cases of diffuse and severe peritoneal tuberculosis in patient with a poor general state of health or in a very weakened state could be a very ominous condition.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
The authors wish to give special thanks to the technical personnel of the Pathology Service of the Hospital General del Sur “Dr. Pedro Iturbe”.
Please cite this article as: González-Ferrer PC, Romero-Amaro ZR, Rivas-Castillo MV, Reyes-Duran PA, Arismendi-Morillo GJ. Tuberculosis peritoneal fibroadhesiva simulando un abdomen agudo inflamatorio por plastrón apendicular. Revista de Gastroenterología de México. 2017;82:261–263.

