
Current guidelines consider endoscopic submucosal dissection (ESD) to be the treatment of choice for most patients with superficial gastric neoplasms with no risk, or very low risk, for lymph node metastasis.1 It enables en bloc resection of tumors larger than 2cm and reliable histologic assessment of the resected specimen to determine the potential curability of the endoscopic resection. In general, the expected scenario after successful ESD is a consolidated and homogeneous scar without any residual tumor, infiltration, or polypoid formation. Interestingly, we have been observing the development of anomalous and bizarre postoperative scars with a relatively large and protruded polypoid nodular neoformation in a subset of patients after curative ESD, particularly for lesions located in the antrum.
The aim of this report was to describe an aberrant polypoid nodular scar (PNS) in a patient after curative ESD and to discuss the theoretical reason for its occurrence.
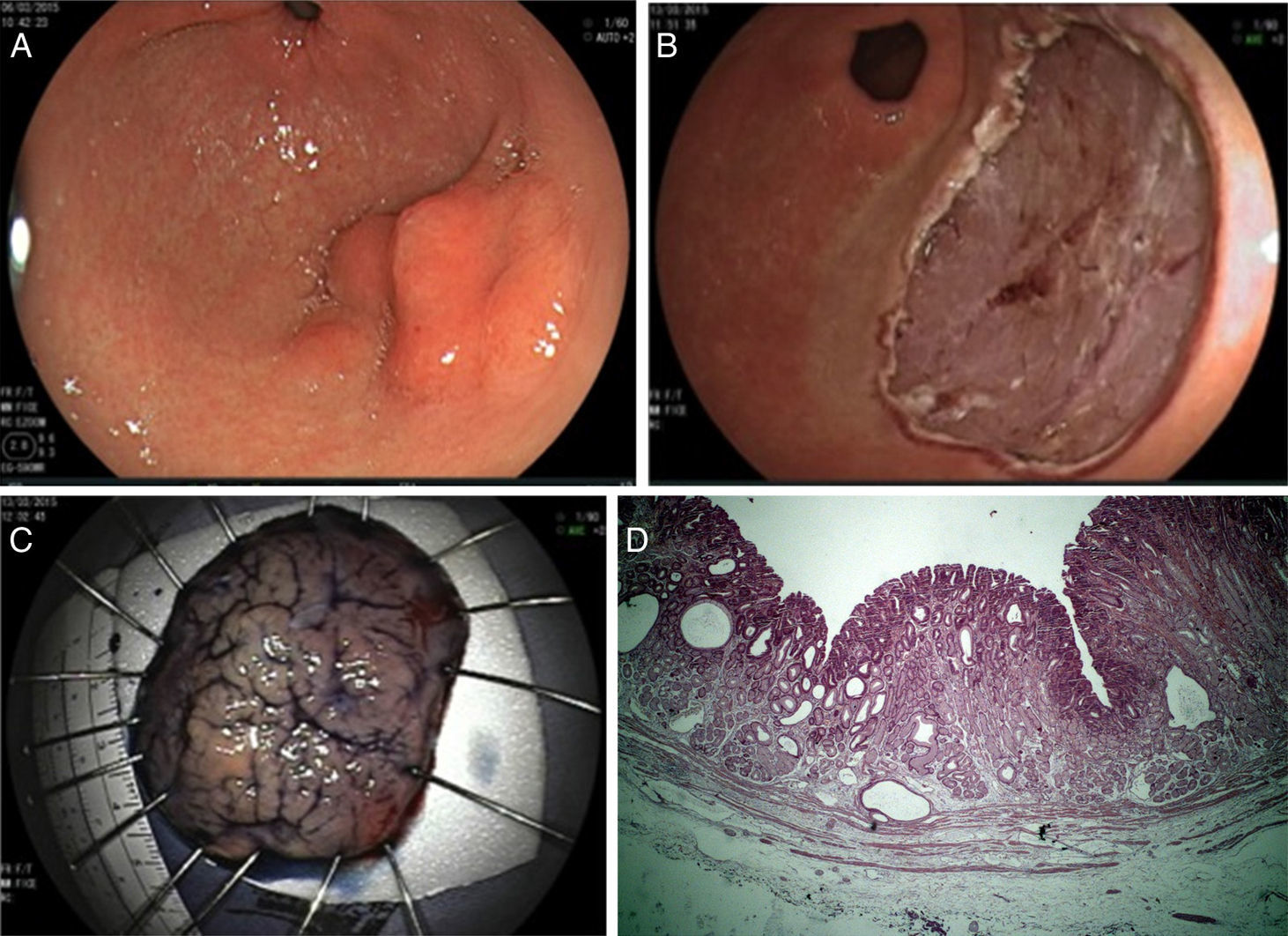
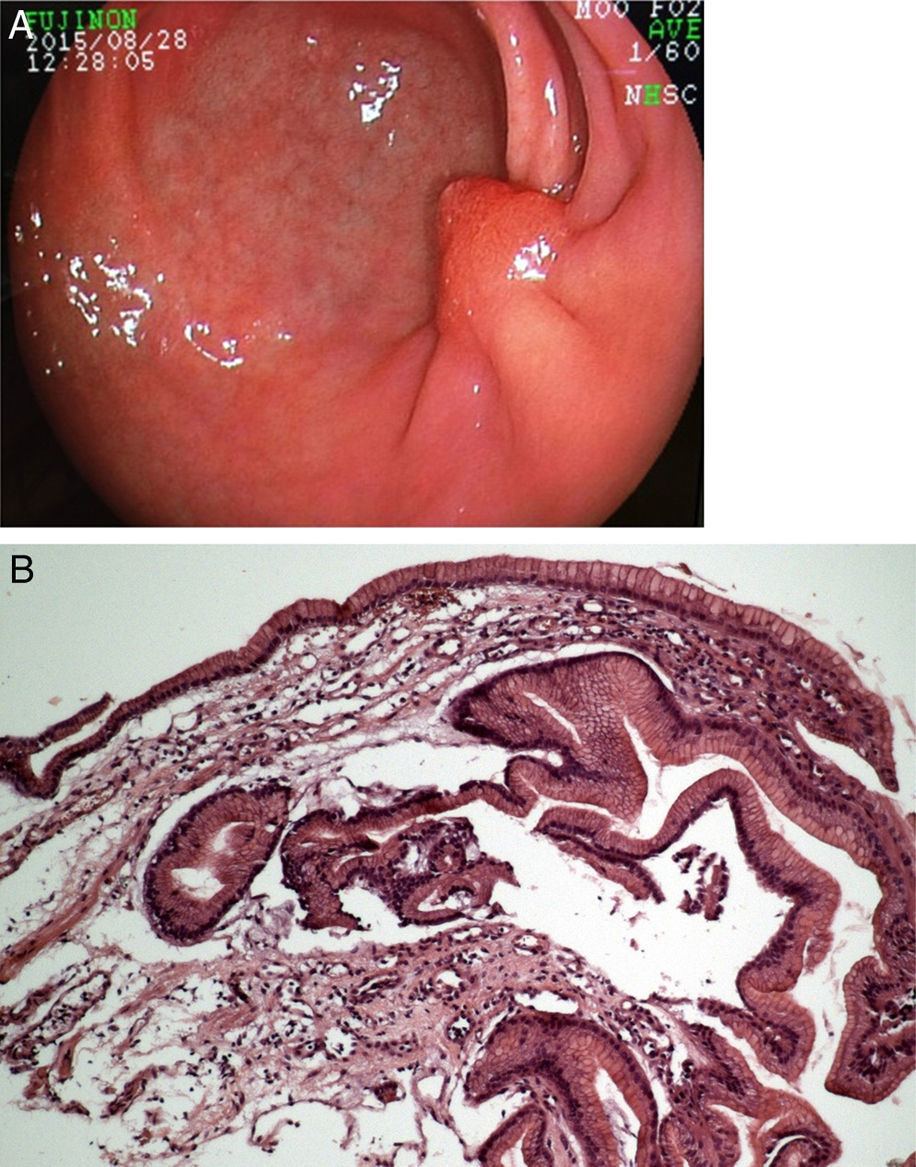
A 53-year-old man was referred to us from another institution. He had a superficially elevated 4-cm lesion with a nodular component and central depression, located in the greater curvature of the antrum (fig. 1A). The preoperative biopsy was consistent with adenoma with low-grade dysplasia. We suspected high-grade dysplasia due to the large size of the lesion and proposed endoscopic en bloc resection by means of ESD. The procedure was carried out under general anesthesia utilizing a single-channel gastroscope (EG-450RD5, Fujifilm Co., Japan) with the water-jet function and a 3.2mm working channel. A transparent 4-mm straight cap was attached to the tip of the endoscope (Elastic Touch®, Top Corporation, Japan). Careful assessment of the tumor borders was carried out with white-light and Flexible Spectral Imaging Color Enhancement (FICE) and the markings were placed 5mm beyond the edges of the tumor. Submucosal (SM) injection was carried out with 0.4% hyaluronic acid (Muco-up®, Johnsons & Johnsons, Japan). ESD was performed with a 2.5mm ball-tipped Flush-Knife (DK2618J-B25, Fujifilm Co., Japan) connected to an electrosurgical generator (VIO® 200D, ERBE Co., Turbingen, Germany) and a water-jet infusion pump (JW-2, Fujifilm Co., Japan). After SM injection with a standard 25-gauge injector needle (Interject, M00518111, Boston Scientific, USA), a circumferential mucosal incision was made outside of the markings (Endocut I, Effect 2, Duration 3, Interval 2). SM dissection was undertaken in the forced coagulation mode (Effect 3, 45 watts), using the cap to expose the submucosa underneath the tumor. Special care was taken to coagulate the perforating vessels (soft coagulation mode, Effect 6, 100 watts). En bloc resection was achieved (fig. 1B) and the specimen was stretched and fixed in a styrofoam plate (fig. 1C). Histologic assessment of the specimen (fig. 1D) confirmed R0 resection, demonstrating a type II foveolar (or pyloric gland) adenoma with high-grade dysplasia limited to the epithelium (M1) with free margins. The postoperative course was uneventful and the patient was kept on 2 weeks of sucralfate and 8 weeks of omeprazole 40mg twice a day. Endoscopic resection was considered curative. According to our protocol for cases such as these, the first endoscopic follow-up is set for 3 to 6 months, and the following ones are annual. Endoscopic control 6 months after the procedure showed convergence of the folds and an aberrant, protruded, polypoid-appearing nodule at the ESD scar (fig. 2A). Local recurrence was strongly suspected, but biopsies revealed regenerative tissue with no dysplasia or adenoma (fig. 2B). The patient was reassured as to the benign characteristics of the scar and advised to undergo annual endoscopic surveillance.
 Type 0IIa+IIc superficial neoplastic lesion in the gastric antrum. B) Endoscopic submucosal dissection with en bloc tumor resection. C) Resected specimen fixed for histologic assessment showing high-grade dysplasia with vertical and lateral free margins and no lymphatic or vascular invasion. D) Histology of the ESD specimen demonstrating type II foveolar adenoma with high-grade dysplasia limited to the epithelium with free lateral and vertical margins.")
A) Type 0IIa+IIc superficial neoplastic lesion in the gastric antrum. B) Endoscopic submucosal dissection with en bloc tumor resection. C) Resected specimen fixed for histologic assessment showing high-grade dysplasia with vertical and lateral free margins and no lymphatic or vascular invasion. D) Histology of the ESD specimen demonstrating type II foveolar adenoma with high-grade dysplasia limited to the epithelium with free lateral and vertical margins.
 Follow-up endoscopy 6 months after ESD, demonstrating fold convergence and an aberrant polypoid nodule at the scar. B) Histology revealed regenerative hyperplastic tissue.")
Ito, et al. reported that a polypoid nodule at the ulcer scar was observed in 12 (6%) of 200 patients with gastric ulcer.2 Interestingly, all lesions were located in the antrum.2 In the past, some of these patients underwent gastric resection because this alteration was suspected to be malignant.3 Due to the development of a polypoid nodule at the ulcer scar, Kato, et al. investigated the gastric ulcer healing process through endoscopy and found that granulation tissue protruded from the healing ulcer in some patients. This was more frequently observed in patients that received a histamine-2 receptor antagonist (H2RA), compared with those treated with drugs other than acid suppressants (22.0% vs 9.7%).4 The protruded granulation tissue developed in 17.5-66.6% of patients with gastric ulcer treated with a proton pump inhibitor (PPI).5,6 This abnormal granulation tissue tended to disappear after scarring, but it remained at the center of the scar for a long period of time in some patients.5,7 The histologic finding of a polypoid nodule at the ulcer scar was reported as hyperplastic regenerative mucosa on the fibrotic tissue.2
Endoscopists should acknowledge the occurrence of aberrant polypoid nodules at the ESD scar, particularly in antral lesions. To the best of our knowledge this has not yet been reported. At our center we have been observing some such findings after ESD for antral tumors. The incidence of this post-ESD phenomenon is still undetermined, but it is expected to be a rare event. PNS endoscopically looks worrisome, especially to the patient or the family physician. However, as long as the ESD procedure was considered a curative R0 resection and scar biopsies rule out recurrence, the PNS should be viewed as a regenerative lesion with an expectedly benign behavior. Over time, the PNS may become less protruded or even disappear and, most importantly, it does not require any type of endoscopic reintervention or surgical management.
Conflict of interestThe authors declare that they have no conflict of interest.
Please cite this article as: Arantes V, Uedo N, Salgado Pedrosa M. Cicatriz nodular polipoide en el antro gástrico después de la disección endoscópica de la submucosa. Revista de Gastroenterología de México. 2017;82:267–269.

