



Colorectal cancer is the most frequent malignant tumor of the digestive system. Its pathogeny is complex and involves the APC/β-catenin sequence. Lymph node metastases are a significant indicator for determining treatment and are a prognostic factor. SOX9 overexpression is related to oncogenic qualities and the capacity for metastasis. Our aim was to analyze SOX9 immunoexpression in primary colorectal cancer and lymph node metastasis status.
Material and methodsSeventy-nine available cases were divided into the group with lymph node metastasis (n=38) and the group without lymph node metastasis (n=41), evaluating their SOX9 expression. The IBM SPSS version 27 program in Spanish was utilized to carry out the statistical analysis, obtaining measures of central tendency, the kappa index, standard deviation, Wilcoxon Mann-Whitney nonparametric measurements, Spearman’s correlation coefficient, and chi-square test and Student’s t test values. SOX9 immunoexpression was evaluated through the mean-based H-score, with high immunoexpression as a score ≥145 and low immunoexpression as a score ≤144.
ResultsA p=0.73 was obtained that was not statistically significant, regarding the relation of SOX9 expression in primary colorectal cancer to lymph node metastasis.
ConclusionsThe absence or presence of lymph node metastasis was independent from SOX9 immunoexpression in primary colorectal cancer. However, due to the limited size of the population analyzed, further research is needed.
El carcinoma colorrectal es la neoplasia maligna más frecuente del sistema digestivo. La patogenia del carcinoma colorrectal es compleja, en la que se encuentra la secuencia APC/β-catenina. Las metástasis a ganglios linfáticos son un indicador significativo para determinar el tratamiento y son factor pronóstico. La sobreexpresión de SOX9 se relaciona con cualidades oncogénicas y capacidad de metástasis. El objetivo fue analizar la inmunoexpresión de SOX9 en el carcinoma colorrectal primario y el estatus de metástasis a ganglios linfáticos.
Material y métodosSe dividieron 79 casos disponibles en los grupos con metástasis a ganglios linfáticos (n=38) sin metástasis a ganglios linfáticos (n=41), en los que se evaluó la expresión de SOX9. Para el análisis estadístico se utilizó el programa IBM SPSS Statistics 27 versión en español para obtener medidas de tendencia central, kappa, desviación estándar y las medidas no paramétricas de Wilcoxon Mann-Whitney y el coeficiente de asociación de Spearman además de las pruebas de chi cuadrado y t de Student. La inmunoexpresión de SOX9 se evaluó mediante H-score en base a la media, como inmunoexpresión alta ≥145 y como baja ≤144.
ResultadosSe obtuvo una P=0.73 el cual no fue significativo en la relación de SOX9 del carcinoma colorrectal primario con las metástasis a ganglios linfáticos.
ConclusionesLa presencia o ausencia de metástasis a ganglios linfáticos es independiente de la inmunoexpresión de SOX9 en el carcinoma colorrectal primario. No obstante, por el número limitado de la población es necesario realizar más investigaciones.
Colorectal cancer is the most frequent tumor of the digestive system and is defined as a malignant tumor of epithelial origin found in the large intestine.1 Regarding its epidemiology, the 2020 Globocan2 reports that colorectal cancer is the third most frequent cancer, following breast cancer, which is in first place, and lung cancer, which is in second place.
In accordance with its glandular formation, colorectal cancer is divided into well differentiated tumors (G1), moderately differentiated tumors (G2), poorly differentiated tumors (G3), and undifferentiated tumors (G4).3 Histologic grade and the TNM classification system of the American Joint Committee on Cancer (eighth edition) are utilized for stratifying this tumor.4
The pathogeny of colorectal cancer is complex and involves diverse genetic and epigenetic mutations. APC/β-catenin sequence alteration is part of the chromosomal instability pathway that is responsible for 65–70% of spontaneous colorectal cancers and the APC mutation, the earliest alteration in colorectal cancer.5
To speak specifically of the molecular biology of metastases in colorectal cancer is to refer to a sequential process. Primary tumors have been described as, composed of multiple genetically distinct subclones.6,7 Authors, such as, Kwak et al., have made proposals for creating new histopathologic parameters that evaluate the stromal microenvironment, predict metastases through the use of artificial intelligence.8
The prognostic factors involved in this cancer include histologic type, tumor stage, the presence of lymphovascular invasion, the presence of tumor budding, host response, the degree of treatment response, surgical margin status, and molecular level of the presence of microsatellite instability and genetic alterations that include APC, TP53, SMDA4, PIK3CA, POLE, BRAF, and RAS1,4,9 of the developmental cancer pathway.
SOX9 in colorectal cancerThe sex determining region Y box-9 protein (SOX9) is a member of the SOX transcription factor family. With respect to its participation in the gastrointestinal tract, studies in vitro have suggested that it participates in Paneth cell differentiation in the intestinal mucosa.10
SOX9 has several implications in colorectal cancer, as both a biomarker in early diagnosis and a prognostic factor. SOX9 has been found to block cell differentiation in the Wnt pathway by activating an enhancer-driven stem cell-like program.11 Likewise, a relation between an increase in tumor budding in stage III and IV tumors, high histologic grade, and strong SOX9 expression has been observed.12 In 2022, Contreras Loera conducted a study at our institution on the association of SOX9 immunoexpression with the differentiation grade of colorectal cancer13 that produced no statistical significance.
SOX9 is associated with other proteins and genes that collaborate with their tumor capacity. Among them is FARSA-AS1, a long non-coding RNA (lnc RNA) gene that is activated by SOX9, which is related to colorectal cancer cell growth and metastases.14 The lncRNA MALAT1/miR-145/SOX9 axis was reported to facilitate colorectal cancer cell proliferation, migration, and tumor invasion.15 The transcriptional activation of FOXK2, mediated by SOX9, also participates in carcinogenesis, promoting tumor activity.16 On the other hand, SOX9 is involved in the prediction of resistance to chemotherapy, through its interaction with DNMT1.17 Claudin-7 is a protein involved in cell adhesion and its low expression was demonstrated through cell cultures, offering improvement in the oncogenic properties of SOX9.18 RAC1 is a transcription factor that can promote the activation of the pentose phosphate pathway of colorectal cancer through SOX9/HK2/G6PD mediation.19 Tumor necrosis factor-associated factor-binding protein domain (ZRANB1) is a deubiquitinase that controls cell growth and metastases, and in turn, increases SOX9 stability by decelerating its ubiquitination.20
Comparable to the development of new therapeutic pathways, authors have conducted studies on the administration of rapamycin (an mTOR inhibitor) in tumors that had a high expression of the biomarker, SOX9.21 Likewise, high levels of SOX9 have been shown to be related to a lower response to treatment with 5-fluorouracil, by increasing vascular invasion and resulting in therapeutic resistance to radiation.22,23
Based on the above, the principal aim of the present study was to evaluate the relation of SOX9 immunoexpression in primary colorectal cancer to lymph node metastasis status.
Material and methodsStudy universe and designAn analytic, observational, cross-sectional study (according to STROBE) was conducted, in which paraffin blocks with a histopathologic diagnosis of colorectal cancer were used. The blocks were archived at the Department of Pathologic Anatomy of the secondary care institution, Hospital Central “Dr. Ignacio Morones Prieto”, in San Luis Potosí, San Luis Potosí, within the time frame of August 1, 2013, to August 31, 2022, providing a total of 79 cases.
Inclusion criteria: all cases that had a histopathologic diagnosis of colorectal cancer, as well as lymph node dissection obtained from intestinal segment resection, were included.
Exclusion criteria: cases with another histopathologic diagnosis, other biopsy specimens, and cases that did not have lymph node dissection were excluded.
Elimination criteria: cases in which the paraffin blocks did not have enough material or did not meet the conditions for performing the immunohistochemical study were eliminated.
The sample size was small (n=79), retrospective, and from a single center for 2 important reasons. The first was the COVID-19 pandemic, which paralyzed the medical care of many patients and their clinical and surgical treatment, resulting in a low number of surgical specimens received at the pathology department; the second was the lack of a more appropriate space for archiving the paraffin blocks, allowing better quality in the conservation of older blocks. Lastly, the release of material requested by the corresponding patient was also a factor.
SOX9 measured by the H-scoreNuclear SOX9 immunoexpression in tumor cells was evaluated in the areas of colorectal cancer corresponding to tumor budding, which were selected by consensus of the 2 reviewing physicians. Good agreement was obtained through the kappa test, with a score of 0.061.
To obtain the H-score, nuclear SOX9 immunoexpression was evaluated by multiplying the percentage of intensity of the tumor cell reaction, by a value ranging from 0 to 3, adding the values for the result, which could range from 0 to 300 (the % of cells with null intensity×0 + % of cells with mild intensity×1 +% of cells with moderate intensity×2 + % of cells with strong intensity×3=0–300).24
The cutoff point was established by obtaining the mean of the total points of the H-score of the 79 cases.13,17 Thus, high immunoexpression was determined as a score ≥145 and low immunoexpression as a score ≤144.
Pilot testBecause the population characteristics were not known, a pilot test was conducted, through randomizing the paraffin blocks utilizing the IBM SPSS version 27 program and calculating the population in 24 cases.25 This resulted in a total of 12 cases with the presence of lymph node metastasis and 12 cases with no lymph node metastasis,25 for the purpose of determining the central tendency values and the behavior of the population. Based on the results, the formula for comparing 2 proportions was then utilized to calculate the sample.26
The demographic aspects, pathologic tumor characteristics, such as location, most common histologic type and grade, tumor size, lymphovascular and perineural invasion, pTNM classification, surgical margins, and clinical characteristics, such as previous treatment, overweight, sedentary lifestyle, smoking, alcoholism, diabetes mellitus, and high blood pressure, were evaluated.
ImmunohistochemistryFor the immunohistochemical study of the paraffin blocks, the EP317 clone SOX9 antibody from BioSB was used, at a 1:200 dilution. The control tissue was the colon and the location of the immunoexpression evaluated was nuclear. The procedure was carried out following the antibody guidelines as described below.
Three slices measuring 3–4 microns were placed on Hydrophilic Plus Slides (BioSB) of the problem case and the respective tissue control. The slides were deparaffinized overnight in an oven at 60°C. They were removed from the oven to cool. Next, the slides were placed in xylene for 10min, passed through absolute alcohol at 96° and 80°, and transferred to distilled water. They were then placed in a decloaking buffer solution (Immuno/DNA Retriever with EDTA, BioSB) and the antigen retrieval procedure was performed in an automated pressure cooker (Decloaking chamber, Biocare). The slides were cooled for 15–20min, then rinsed for 5min with distilled water and placed in hydrogen peroxide (3%) for 15min. Once again, they were rinsed with distilled water for 5min. They were placed in TBS with Tween and the slices were covered with the SOX9 antibody (100μl). They were placed in a humidified chamber and incubated for 30–40min. The SOX9 antibody was diluted with TBSt, following the antibody dilution indications of 1:200, and rinsed with abundant TBSt. The slides were covered with biotinylated secondary antibody (biotin link) for 10min and again rinsed with abundant TBSt. They were then covered with polymers (-streptavidin-HRP) for 10min and rinsed with abundant TBSt. Peroxidase activity was revealed under control microscopy, utilizing diaminobenzidine. The reaction was stopped by placing the slices in distilled water. Counterstaining was carried out with Harris hematoxylin for 30s. Lastly, the slides were rinsed with running water, then in distilled water, and finally dehydrated until xylene to be covered with Entellan®.
Statistical analysisThe IBM SPSS version 27 program in Spanish was used for the statistical analysis. Measures of central tendency were determined for the quantitative variables of the study.27 The mean was calculated for the age variable and the mode was calculated for the frequency of sex, histologic type, and location. Variability was calculated through standard deviation and the kappa formula was applied to measure the concordance of the results of the 2 physicians that evaluated the H-score of the slides. With respect to the population characteristics, the chi-square test was utilized to evaluate previous treatment and sedentary lifestyle, in relation to the expression levels determined by the H-scores. The Shapiro-Wilk, Levene’s, and Student’s t tests were used in the cases of alcoholism, smoking, overweight, diabetes mellitus, and high blood pressure.
The nonparametric Wilcoxon Mann–Whitney and Spearman’s correlation coefficient tests were utilized to determine the difference between the lymph node metastasis group and the group with no lymph node metastasis. Lastly, the Levene’s test for homogeneity of variance, based on the mean, was performed.
Ethical considerationsThe present study was no risk for patients, given that they were not directly involved. They only provided the histopathologic material with no immediate additional intervention.
The data were managed by numbers assigned to the material by the institution, maintaining strict confidentiality of the available information. The data were produced in accordance with Mexican Federal Law for the protection of personal data held by individuals.
After reviewing the Norma Oficial Mexicana NOM-004-SSA3-2012 of the Clinical Case Record and the Declaration of Helsinki, the study was deemed to have no risk for the patients involved. It was approved by the Ethics and Research Committee of the Hospital Central “Dr. Ignacio Morones Prieto” and assigned registry number 86−22.
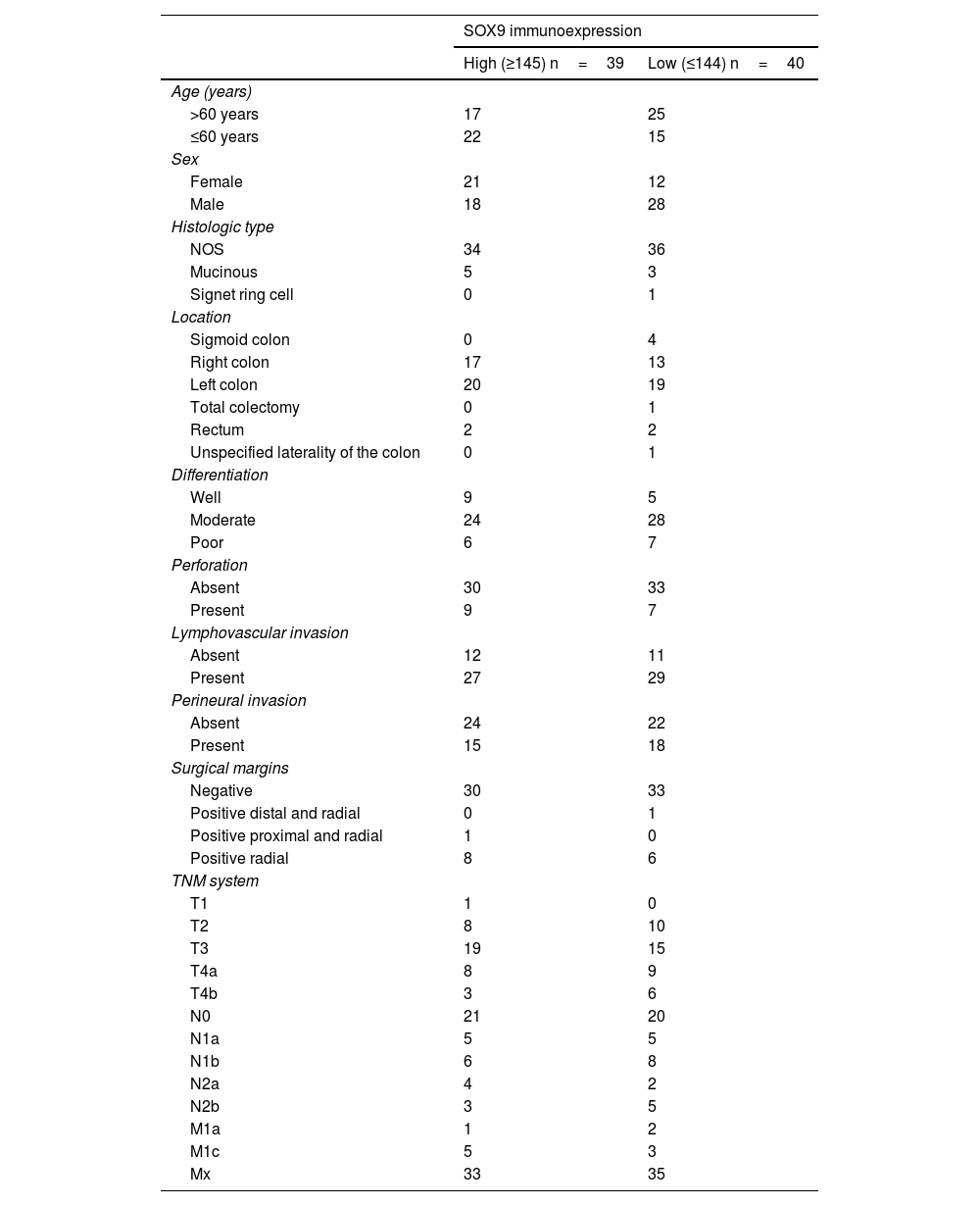
ResultsPopulation characteristicsThe population characteristics and risk factors related to patient SOX9 expression and lymph node status, were analyzed. Starting with age, a mean of 60 years at colorectal cancer presentation was obtained; 37 of those patients were under 60 years of age and 42 were older than 60 years of age. Of the patients under 60 years of age, 22 had high SOX9 immunoexpression (10 with lymph node metastasis and 12 without), compared with 17 of the patients above 60 years of age (8 with lymph node metastasis and 9 without). Fifteen of the patients under 60 years of age had low SOX9 expression (9 with lymph node metastasis and 6 without), compared with 25 cases in the patients above 60 years of age (11 with lymph node metastasis and 14 without). As a point of interest, 6 cases of patients under 40 years of age were identified. Five of them had high SOX9 expression (3 with lymph node metastasis and 2 without) and one had low SOX9 expression and no lymph node metastasis.
Regarding sex, of the 79 cases, 46 were men and 33 were women. Table 1 shows the relation between SOX9 immunoexpression and sex.
With respect to histologic type, 70 cases (88.6%) corresponded to NOS adenocarcinoma (previously known as intestinal adenocarcinoma), 8 cases (10.1%) to mucinous adenocarcinoma, and one case (1.2%) to signet cell adenocarcinoma.
Regarding location, the tumor was found in the left colon in 43 cases; 20 of those cases had high SOX9 expression (8 with lymph node metastasis and 12 without) and 23 cases had low SOX9 expression (12 with lymph node metastasis and 11 without). Tumor was located in the right colon in 30 cases; 17 of them had high SOX9 expression (9 with lymph node metastasis and 8 without) and 13 had low SOX9 expression (6 with lymph node metastasis and 7 without). Tumor was located in the rectum in 4 cases; 2 had high SOX9 expression (one with lymph node metastasis and one without) and 2 had low SOX9 expression (both with no lymph node metastasis). One patient with total colectomy had low SOX9 immunoexpression and no lymph node metastasis, and one patient had unspecified tumor location, low SOX9 expression, and no lymph node metastasis.
With respect to differentiation grade, 14 cases corresponded to well differentiated colorectal cancer; 9 of those cases had high SOX9 immunoexpression (3 with lymph node metastasis and 6 without) and 5 had low SOX9 expression (all 5 without lymph node expression). Fifty-two cases corresponded to moderately differentiated tumor; 24 cases had high SOX9 expression (13 with lymph node metastasis and 11 without) and 28 had low SOX9 expression (17 with lymph node metastasis and 11 without). Lastly, 13 cases presented with poorly differentiated tumor; 6 had high SOX9 expression (2 with lymph node metastasis and 4 without) and 7 had low SOX9 expression (3 with lymph node metastasis and 4 without).
Tumor size was reported at a mean total of 6.13cm, the smallest of which was 1cm and the largest 17cm. No tumor size was reported for 2 cases because the slide review came from an external laboratory.
Perforation was present in 16 of the 79 colorectal cancer cases; 9 of those cases had high SOX9 expression (6 with lymph node metastasis and 3 without) and 7 had low SOX9 expression (4 with lymph node metastasis and 3 without). There was no perforation in the remaining 63 cases; 30 of those patients had high SOX9 expression (12 with lymph node metastasis and 18 without) and 33 had low SOX9 expression (16 with lymph node metastasis and 17 without).
With respect to lymphovascular invasion, it was present in 56 of the 79 cases and absent in 23. Of the 56 cases with invasion, 27 had high SOX9 expression (15 with lymph node metastasis and 12 without) and 29 had low SOX9 expression (19 with lymph node metastasis and 10 without). Of the 23 cases with no invasion, 12 had high SOX9 expression (3 with lymph node metastasis and 9 without) and 11 had low SOX9 expression (one with lymph node metastasis and 10 without).
Perineural invasion was present in 33 cases; 15 had high SOX9 expression (9 with lymph node metastasis and 6 without) and 18 had low SOX9 expression (11 with lymph node metastasis and 7 without). Of the 46 remaining cases, 24 had high SOX9 expression (9 with lymph node metastasis and 15 without) and 22 had low SOX9 expression (9 with lymph node metastasis and 13 without).
With respect to surgical margins, 63 cases had negative margins; 33 of them had high SOX9 expression (16 with lymph node metastasis and 17 without) and 30 had low SOX9 expression (10 with lymph node metastasis and 20 without). There was one case with positive distal and radial surgical margins, low SOX9 expression, and lymph node metastasis, as well as one case with positive proximal and radial margins, high SOX9 expression, and lymph node metastasis. The remaining 14 cases had a positive radial margin; 8 of those cases had high SOX9 expression (7 with lymph node metastasis and one without) and 6 had low SOX9 expression (3 with lymph node metastasis and 3 without).
TNM system classification was the following: regarding the extent of the tumor (T), there was one case with T1, high SOX9 expression, and no lymph node metastasis; 18 cases were T2, 8 of which had high SOX9 expression (one with lymph node metastasis and 7 without) and 10 had low SOX9 expression (4 with lymph node metastasis and 6 without); 34 cases were T3, 19 of which had high SOX9 expression (10 with lymph node metastasis and 19 without) and 15 had low SOX9 expression (8 with lymph node metastasis and 7 without); T4 was subdivided into T4a and T4b, and there were 17 cases of T4a, 8 of which had high SOX9 expression (5 with lymph node metastasis and 3 without) and 9 with low SOX9 expression (4 with lymph node metastasis and 5 without) and 9 cases of T4b, 3 of which had high SOX9 expression (2 with lymph node metastasis and one without) and 6 with low SOX9 expression (4 with lymph node metastasis and 2 without). The results for the extent of spread to lymph nodes (N) were commented on above. With respect to the presence of metastasis (M), 11 cases were identified during follow-up with histopathologic studies reporting suspected metastasis to other organs and cases of metastasis to the peritoneal surface. Three cases were identified as M1a, one with high SOX9 expression (with lymph node metastasis) and 2 with low SOX9 expression (one with lymph node metastasis and one without). Eight cases were identified as having M1c, 5 of which had high SOX9 expression (4 with lymph node metastasis and one without) and 3 with low SOX9 expression (all with lymph node metastasis). The 68 remaining cases were reported as Mx due to a lack of information necessary to make the classification. The data are described in Table 2.
Population characteristics.
| SOX9 immunoexpression | ||
|---|---|---|
| High (≥145) n=39 | Low (≤144) n=40 | |
| Age (years) | ||
| >60 years | 17 | 25 |
| ≤60 years | 22 | 15 |
| Sex | ||
| Female | 21 | 12 |
| Male | 18 | 28 |
| Histologic type | ||
| NOS | 34 | 36 |
| Mucinous | 5 | 3 |
| Signet ring cell | 0 | 1 |
| Location | ||
| Sigmoid colon | 0 | 4 |
| Right colon | 17 | 13 |
| Left colon | 20 | 19 |
| Total colectomy | 0 | 1 |
| Rectum | 2 | 2 |
| Unspecified laterality of the colon | 0 | 1 |
| Differentiation | ||
| Well | 9 | 5 |
| Moderate | 24 | 28 |
| Poor | 6 | 7 |
| Perforation | ||
| Absent | 30 | 33 |
| Present | 9 | 7 |
| Lymphovascular invasion | ||
| Absent | 12 | 11 |
| Present | 27 | 29 |
| Perineural invasion | ||
| Absent | 24 | 22 |
| Present | 15 | 18 |
| Surgical margins | ||
| Negative | 30 | 33 |
| Positive distal and radial | 0 | 1 |
| Positive proximal and radial | 1 | 0 |
| Positive radial | 8 | 6 |
| TNM system | ||
| T1 | 1 | 0 |
| T2 | 8 | 10 |
| T3 | 19 | 15 |
| T4a | 8 | 9 |
| T4b | 3 | 6 |
| N0 | 21 | 20 |
| N1a | 5 | 5 |
| N1b | 6 | 8 |
| N2a | 4 | 2 |
| N2b | 3 | 5 |
| M1a | 1 | 2 |
| M1c | 5 | 3 |
| Mx | 33 | 35 |
Summary of the characteristics of the population with colorectal cancer per group by H-score determination of SOX9 expression.
In relation to the clinical data of treatment prior to surgery, sedentary lifestyle, overweight, smoking, alcoholism, and the chronic and degenerative diseases of diabetes mellitus and high blood pressure, due to regulatory issues regarding the safeguarding of hospital clinical records, the information was only available up to 5 years before the present study. As a consequence, only the data corresponding to the 57 cases (n=57) seen during that period of time were obtained.
Previous treatment in the patients with colorectal cancer was reported in 3 of the 57 cases; one patient received chemotherapy prior to surgery and the remaining 2 received both radiotherapy and chemotherapy. Two cases had high SOX9 expression without lymph node metastasis and the remaining case had low SOX9 expression and lymph node metastasis. The tumor was located in the left colon in 2 of the cases with previous treatment and in the rectum in the remaining case. Fifty-four cases had no previous treatment; 23 of them had high SOX9 expression (10 with lymph node metastasis and 13 without) and 31 had low SOX9 expression (16 with lymph node metastasis and 15 without). The H-score variables (high and low) with previous treatment (absent and present) were evaluated using the chi-square test, producing statistical significance with a p of 0.413.
A sedentary lifestyle was identified in 2 cases and absent in 55. Of those 2 cases, one had high SOX9 expression, and one had low SOX9 expression; neither of them had lymph node metastasis. Twenty-four of the 55 cases had high SOX9 expression (10 with lymph node metastasis and 14 without) and 31 of the cases had low SOX9 expression (17 with lymph node metastasis and 14 without). The chi-square evaluation of the relation between sedentary lifestyle and SOX9 expression produced a p of 0.859.
Smoking was present in 7 cases and absent in 50. Two of the 7 cases had high SOX9 expression (one with lymph node metastasis and one without) and 5 had low SOX9 expression (3 with lymph node metastasis and 2 without). Of the 50 cases, 23 had high SOX9 expression (9 with lymph node metastasis and 14 without) and 27 had low SOX9 expression (14 with lymph node metastasis and 13 without). The Shapiro–Wilk test produced a p of 0.196 and 0.933, indicating normal data distribution. Later, the Levene’s test based on a mean of 0.694 and the Student’s t test produced a statistically significant (assuming equal variances) p of 0.421.
Alcoholism was present in 6 cases, and according to the clinical records, was absent in 51. Two of the 6 cases had high SOX9 expression (one with lymph node metastasis and one without) and 4 had low SOX9 expression (3 with lymph node metastasis and one without. Of the 51 cases, 23 had high SOX9 expression (9 with lymph node metastasis and 14 without) and 28 had low SOX9 expression (14 with lymph node metastasis and 14 without). The Shapiro–Wilk test produced a p of 0.225 and 0.148. The Levene’s test based on the mean produced a p of 0.958 and the Student’s t test produced a p of 0.389.
Overweight was present in 7 cases and absent in 50. Of the 7 cases, 2 had high SOX9 expression (both with lymph node metastasis) and 5 had low SOX9 expression (4 with lymph node metastasis and one without). Of the 50 cases, 23 had high SOX9 expression (8 with lymph node metastasis and 15 without) and 27 had low SOX9 expression (13 with lymph node metastasis and 14 without). The Shapiro-Wilk test produced a p of 0.178 and 0.578. The result of the Levene’s test based on the mean was 0.320 and the Student’s t test produced a p of 0.489.
High blood pressure was present in 14 cases and absent in 43. Of the 14 cases, 5 had high SOX9 expression (4 with lymph node metastasis and one without) and 9 had low SOX9 expression (5 with lymph node metastasis and 4 without). Of the 43 cases, 20 had high SOX9 expression (6 with lymph node metastasis and 14 without) and 23 had low SOX9 expression (12 with lymph node metastasis and 11 without). The results of the Shapiro-Wilk test were a p of 0.318 and 0.546 and the results of the Levene’s test and the Student’s t test were 0.235 and 0.230, respectively.
Diabetes mellitus was present in 12 cases and absent in 45. In the 12 cases with diabetes mellitus, 6 had high SOX9 expression (4 with lymph node metastasis and 2 without) and 6 had low SOX9 expression (4 with lymph node metastasis and 2 without). Of the 45 cases with no diabetes mellitus, 19 had high SOX9 expression (6 with lymph node metastasis and 13 without) and 26 had low SOX9 expression (13 with lymph node metastasis and 13 without). The Shapiro-Wilk test produced a p of 0.434 and 0.725, the Levene’s test based on the mean produced a p of 0.468, and the Student’s t test produced a p of 0.766.
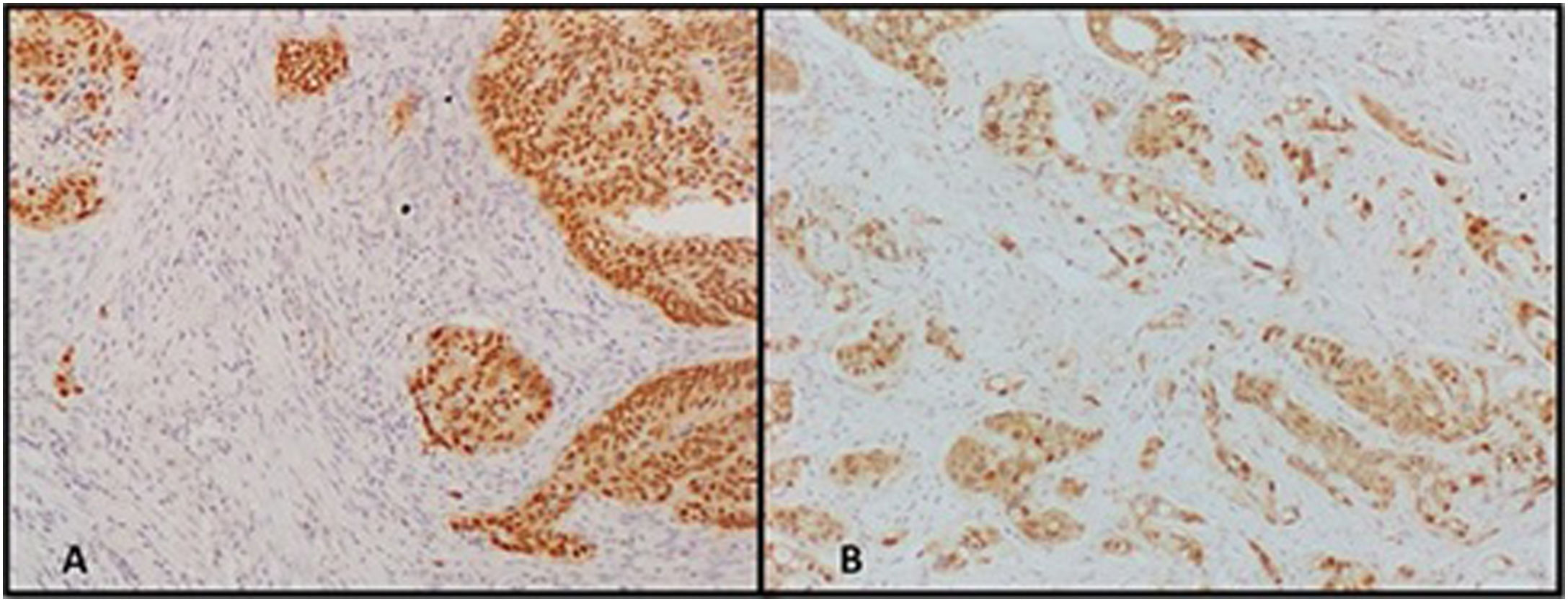
SOX9 immunoexpression and lymph node metastasisThe 79 cases analyzed were divided into 2 groups: the group with lymph node metastasis (n=38) and the group without lymph node metastasis (n=41). Fig. 1 shows the nuclear SOX9 immunoexpression measured by the H-score.
 High nuclear SOX9 expression (H-score ≥ 145). (B) Low nuclear SOX9 expression (H-score ≤ 144). Photomicrographs of the colon showing nuclear SOX9 antibody expression. Image A is an example of high nuclear marking and image B is an example of low nuclear expression.")
Nuclear staining of SOX9 in the colon with high and low expression determined through the H-score. (A) High nuclear SOX9 expression (H-score ≥ 145). (B) Low nuclear SOX9 expression (H-score ≤ 144). Photomicrographs of the colon showing nuclear SOX9 antibody expression. Image A is an example of high nuclear marking and image B is an example of low nuclear expression.
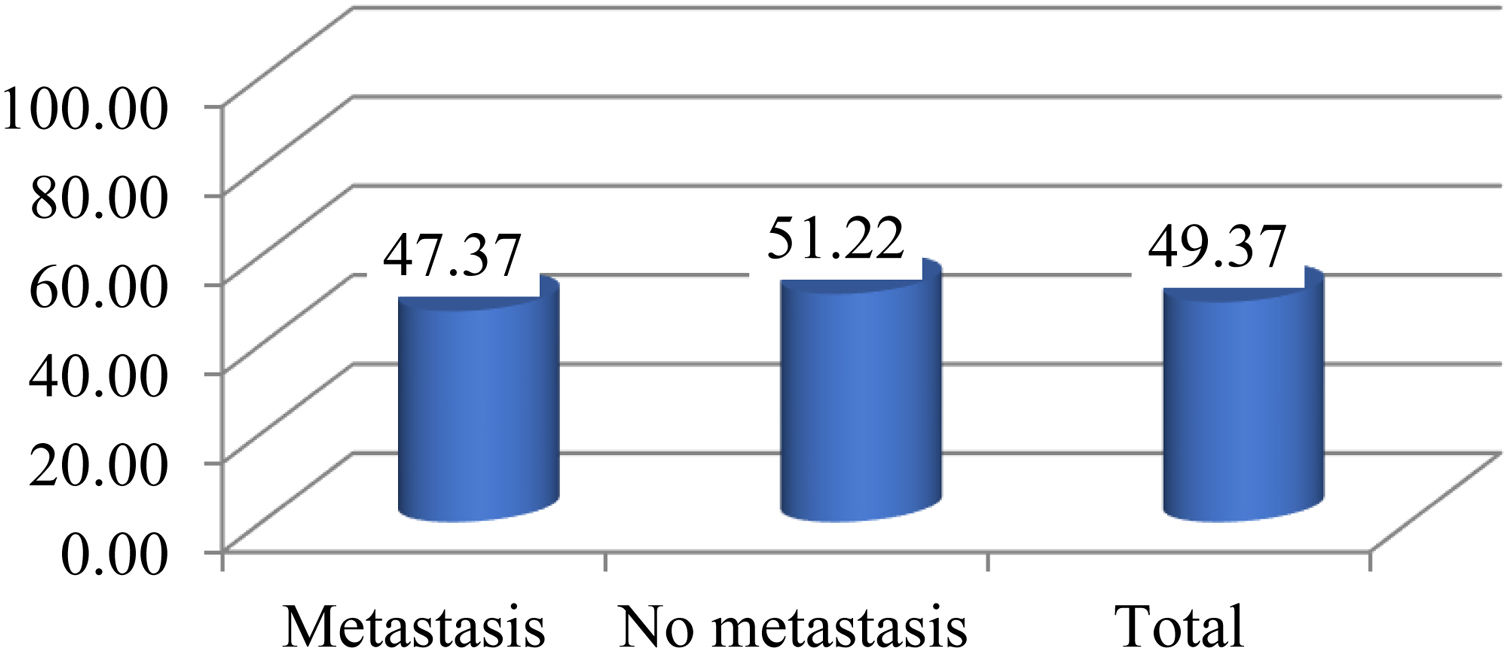
Regarding high SOX9 immunoexpression, from a total of 39 cases, 18 (47%) corresponded to the group with lymph node metastasis and 21 (51%) to the group without lymph node metastasis (Fig. 2).
 and the group with no lymph node metastasis (51%). The bar graph shows the cases with high SOX9 immunoexpression divided into the group with lymph node metastasis and the group with no lymph node metastasis.")
Distribution represented in percentages of cases with high SOX9 immunoexpression in the group with lymph node metastasis (47%) and the group with no lymph node metastasis (51%). The bar graph shows the cases with high SOX9 immunoexpression divided into the group with lymph node metastasis and the group with no lymph node metastasis.
With respect to the 40 cases that had low SOX9 expression, 20 cases presented with lymph node metastasis and 20 did not. The results of the 2 groups produced a p of 0.73, as shown in Table 3.
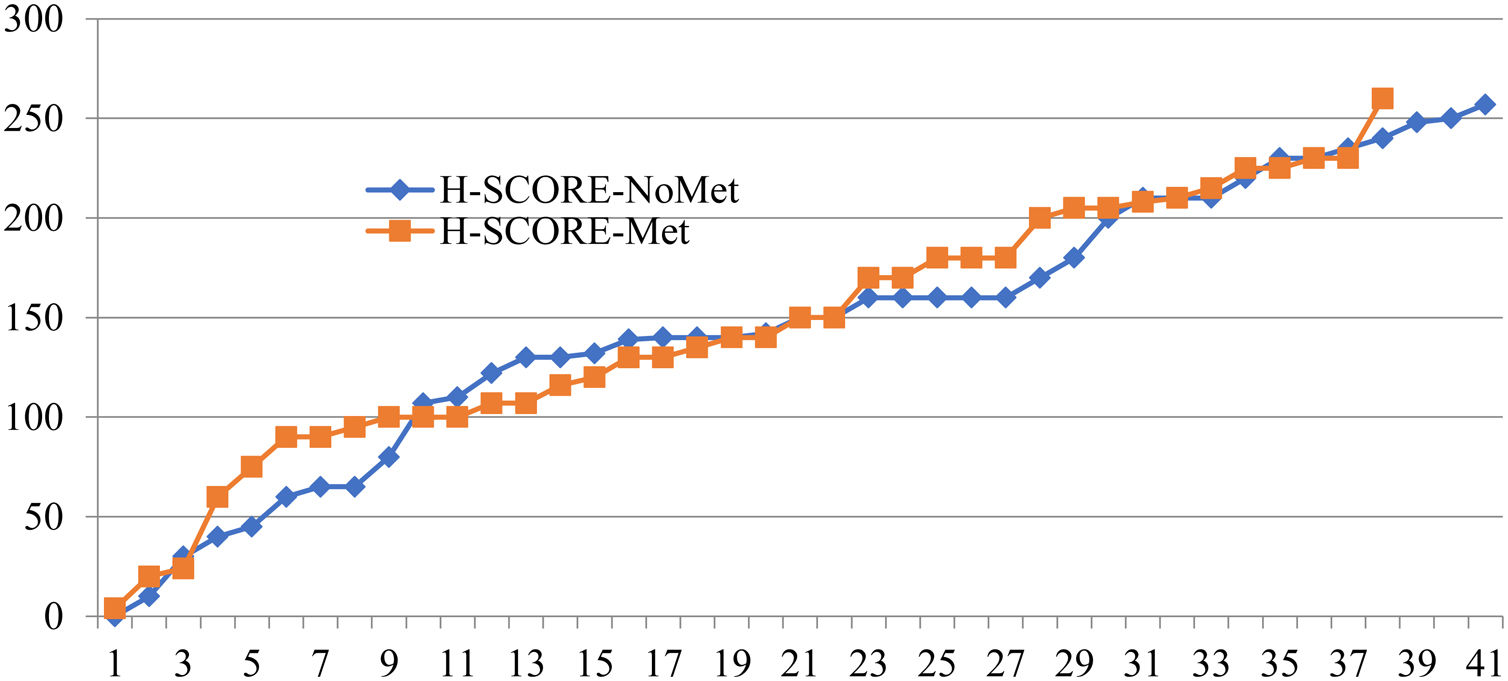
Fig. 3 demonstrates a similar H-score value distribution trajectory in the cases with high SOX9 expression.
 in the groups with and without lymph node metastases, showing very similar value distribution in the metastasis group (orange line) and the group with no metastasis (blue line).")
Regarding N of the TNM system, 41 cases were N0 and the 38 cases that had lymph node metastasis were classified as follows: 10 cases were N1a, 5 with high SOX9 expression and 5 with low SOX9 expression; 14 cases were N1b, 6 with high SOX9 expression and 8 with low SOX9 expression; 6 cases were N2a, 4 with high SOX9 expression and 2 with low SOX9 expression; and 8 cases were N2b, 3 with high SOX9 expression and 5 with low SOX9 expression.
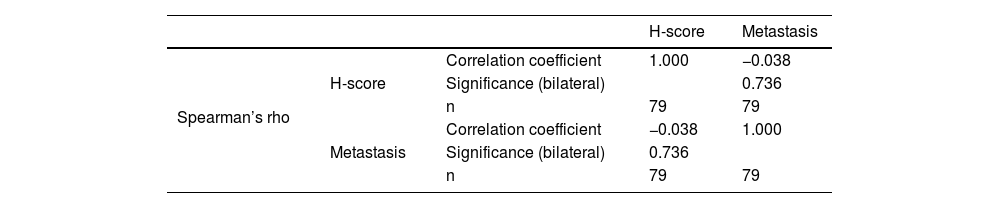
Nonparametric testsThe Spearman’s correlation coefficient and Wilcoxon Mann-Whitney tests were carried out to determine the difference between the 2 groups analyzed. The Spearman’s test resulted in a p of 0.73 and a correlation coefficient of –0.038 (Table 4).
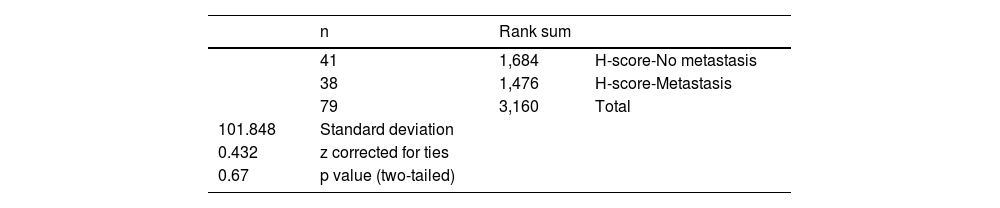
The result of the Wilcoxon Mann-Whitney test was a p of 0.67, with a standard deviation of 101.848 (Table 5).
The Levene’s test for homogeneity of variance based on the previously presented variances resulted in a p of 0.868, as shown in Table 6.
The Levene’s test for homogeneity of variance.
| Levene’s statistic | df1 | df2 | Significance | ||
|---|---|---|---|---|---|
| H-score | Based on the mean | 0.028 | 1 | 77 | 0.868 |
The Levene’s test for homogeneity of variance based on the mean, with a p of 0.868, indicating that the variances are not significantly different from each other.
Colorectal cancer has high incidence and mortality rates, and so there is a search for the identification of prognostic factors to guide treatment and the development of new therapies. The different prognostic factors for colorectal cancer include the presence of lymph node metastasis. Proposals have been described in the literature for predicting lymph node metastasis through different tools, such as molecular biology and cell cultures; even the use of artificial intelligence has been included for that purpose, and in turn, to detect cancer at earlier stages.7,9,11,14,15
As mentioned above, SOX9 is a transcription factor that has been related to the maintenance of stem cells. It participates in tissue homeostasis and in tumor regeneration and development, and is overexpressed in various tumors, including colorectal cancer. Likewise, 5–10% of cases present with a gene mutation, and even though SOX9 has a dose-dependent effect on the epithelial cells of the intestine, in metastases, it appears to act independently of that effect. Studies have been performed on cell cultures,20,21 with other techniques of molecular pathology, such as immunohistochemistry, but nothing has been described at present.
The limitations of the present study were the small sample size, its retrospective design, and the fact that it was conducted at a single center. The COVID-19 pandemic paralyzed the medical attention of many patients, including their clinical and surgical treatment. This resulted in a low number of surgical specimens sent to the pathology department. The presence of microsatellite instability as an additional study variable could not be evaluated due to the lack of resources needed for its analysis.
With respect to population characteristics and risk factors, the left colon was the most common site of colorectal cancer location. The mean age of the patients was 60 years, with a higher incidence in patients above that age. Male sex was the most affected (46 of the 79 cases: 58%), with a predominance of low SOX9 expression. These observations are in line with previous descriptions in the literature.
Intestinal perforation of colorectal cancer was present in a minority of patients (16 of the 79 cases: 20%), raising the risk of progression and tumor spread. Lymphovascular invasion was more frequent than perineural invasion. Surgical margins were negative in the majority of cases. Regarding the TNM system, the most frequent T was T3 for tumor size. On the other hand, in the N category, 41 cases were N0 (negative cases) and 38 cases were positive, the most recurrent of which was N1b. For M, the lack of clinical data regarding metastasis was a limitation. Only the cases whose biopsies of distant organs were sent to the pathology department were registered, and information was provided for very few cases.
Due to the NOM-004-SSA3-2012 clinical record regulation, the data on treatment before surgery and the personal history of alcoholism, smoking, sedentary lifestyle, overweight, diabetes mellitus, and high blood pressure were only available up to 5 years before the start of our study. Nevertheless, it could be concluded that the majority of cases did not receive previous treatment because the majority of patients were admitted with symptoms of acute abdomen, requiring immediate surgical management.
ConclusionsThere was no correlation between SOX9 immunoexpression and the presence of metastasis, upon obtaining a p of 0.73, indicating that the presence or absence of lymph node metastasis is independent from SOX9 immunoexpression. There was no statistically significant difference between the 2 groups (metastasis and no metastasis) and SOX9 immunoexpression. Likewise, SOX9 immunoexpression was independent from the histopathologic characteristics of colorectal cancer, its histologic grade, and its stratification according to the pTNM and there was no relation between SOX9 and the clinical data analyzed in the study population, results validated by a p with no statistical significance, obtained from the chi-square test and Student’s t test. However, further research studies need to be carried out.
Financial disclosureFinancing was obtained through the Universidad Autónoma de San Luis Potosí (UASLP). The SOX9 antibody is included among the antibodies belonging to the immunohistochemistry laboratory of the UASLP given that it is a routinely used antibody.
Conflict of interestThe authors declare there is no conflict of interest.
The authors wish to thank the Q.F.B., Susana de los Ángeles Chávez Porras, at the immunohistochemistry laboratory of the Universidad Autónoma de San Luis Potosí and the Q.F.B., Angélica Ma. Esquivel Ojeda, at the Hospital Central “Dr. Ignacio Morones Prieto”, who performed the immunohistochemical techniques. Likewise, we wish to thank the personnel of the Universidad Autónoma de San Luis Potosí and the Pathologic Anatomy Department of the Hospital Central “Dr. Ignacio Morones Prieto” for their collaboration in carrying out this work.

