
Gastric pneumatosis (GP) is defined as the presence of gas within the gastric wall. It can be comprised of 2 entities with different etiologies, symptoms, and outcomes: gastric emphysema (GE) and emphysematous gastritis (EG).1 GE is usually asymptomatic and generally secondary to mechanical causes.2 EG is secondary to an infection in the gastric wall due to gas-producing microorganisms. GE does not require surgical treatment and generally responds to conservative management,3 but EG requires more aggressive treatment that includes the use of antibiotics, and in some cases, surgery, with a high mortality rate.
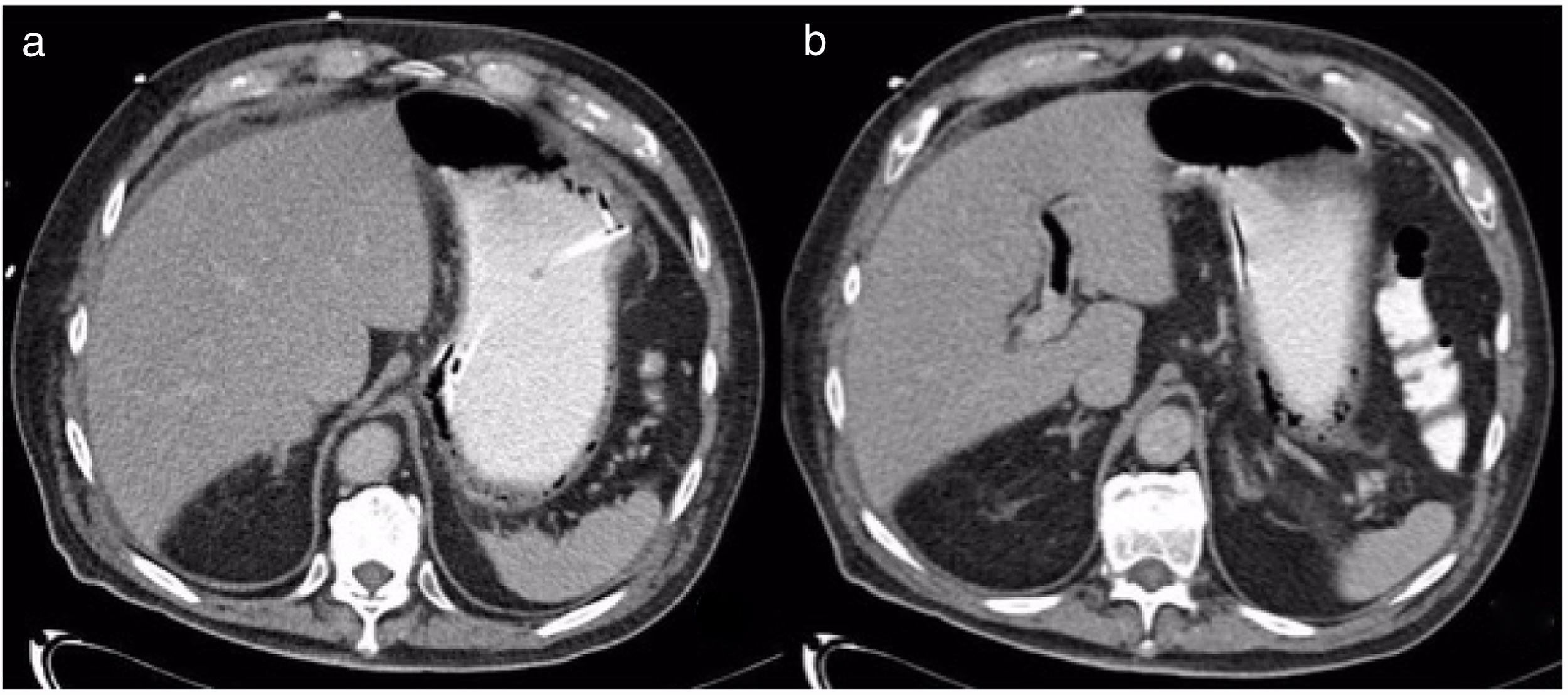
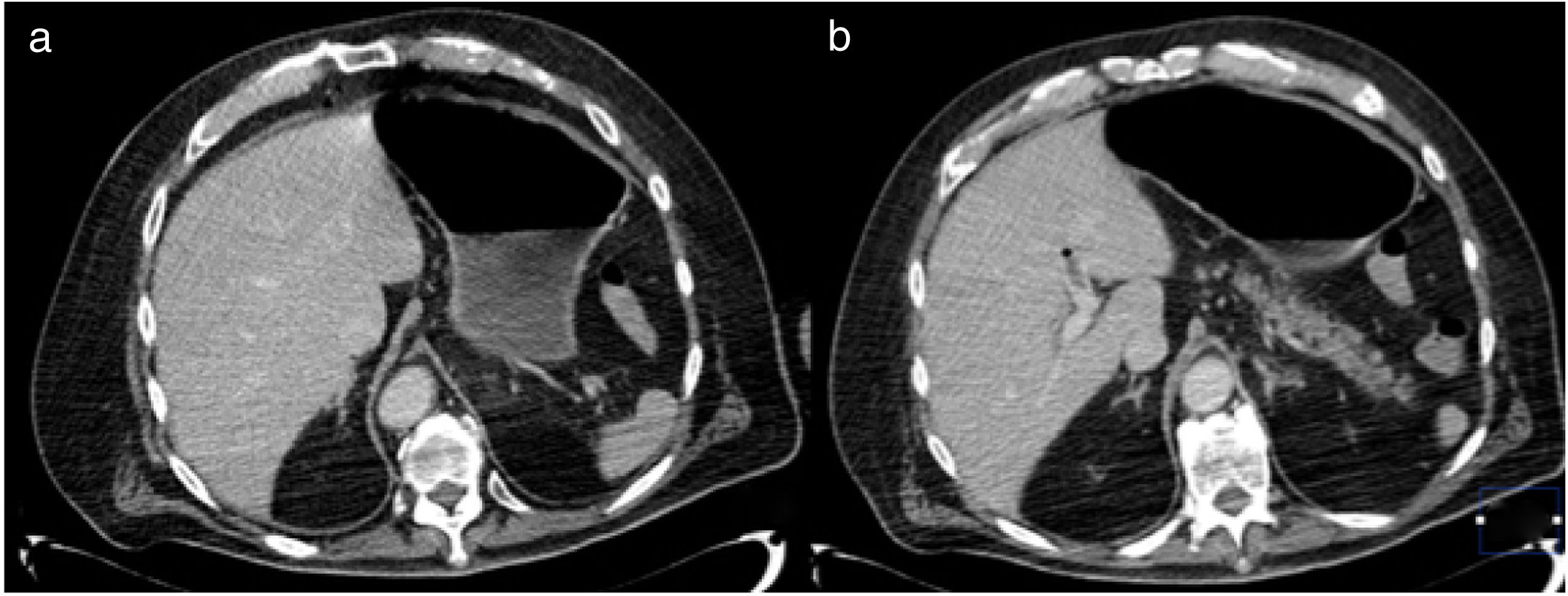
We present herein the case of a patient with gastric pneumatosis and portal vein gas that was treated conservatively. A 76-year-old man was diagnosed with high blood pressure and chronic kidney disease. He was admitted to the intensive care unit due to community-acquired pneumonia and acute respiratory failure. Nasogastric feeding was begun. Four days later, he presented with abdominal distension and diarrhea. An abdominal x-ray revealed dilation of the gastric chamber, with no dilation of the intestinal segments. An abdominal CAT scan identified pneumatosis in the distal third of the esophagus and the stomach and gas in the left portal vein (fig. 1). Angiotomography showed vascular structure permeability. Enteral feeding was suspended for one day, and then resumed, with no abdominal distension. A control CAT scan performed 5 days later demonstrated reduced gas in the portal vein and absence of gastric pneumatosis (fig. 2). The patient's pneumonia progressed, requiring mechanical ventilation, as well as kidney replacement therapy, and he died 7 days after the diagnosis of pneumatosis.
 CAT scan showing gastric pneumatosis and the presence of the enteral catheter adjacent to the gastric wall; b) Evidence of gas in the branch of the left portal vein.")
 CAT scan showing no evidence of abnormal thickening of the stomach, and resolution of the pneumatosis can be seen; b) Decrease in portal vein gas, with the presence of a thrombus in the left branch.")
GP is not a diagnosis, but rather a radiologic finding that can be the result of different pathologic processes.4 The significance of GP depends on its nature and the severity of the underlying condition, which can range from benign diseases to abdominal sepsis, leading to death.
GE is usually a benign condition resulting from disruption of the mucosa. The main causes are obstruction of gastric emptying, increased intraluminal pressure, duodenal obstruction, nonsteroidal analgesics, alcohol, steroids, instrumentation, lung bullae rupture, pneumothorax, or prolonged CPR.5 Clinical manifestations tend to be nonspecific: epigastric pain, bloating, nausea, vomiting, hematemesis, or melena.
EG is the product of gas-producing bacterial invasion through the gastric wall. The most frequent bacteria are K. pneumoniae, E. coli, Enterobacter spp, and P. aeruginosa.6 The main predisposing factor is diabetes mellitus. Clinical manifestations are not different from those in GE, but patients with EG frequently present with fever and altered alert status. In addition, elevated lactate and creatinine levels are related to increased mortality.
CAT is the diagnostic study of choice. Some of the findings related to GP are portal vein gas, intestinal pneumatosis, or pneumoperitoneum, and are present in 41% of the cases of EG and 33% of the cases of GE.3 Gastric mucosa ischemia may be present in half of the patients with EG that undergo endoscopy.4 Initial treatment for both entities is fluid resuscitation, fasting, gastric decompression, and broad-spectrum antibiotics, in case of signs of infection.3 Endoscopy should be performed, and if ischemia of the mucosa is documented, surgical treatment should be considered.
In the present case, a mechanical origin of the GP, secondary to trauma, is suggested, due to the fact that a nasogastric catheter was placed, and gastric distension presented. GP is a radiologic finding with two opposing clinical outcomes. Once detected, it is decisive to establish whether the condition is due to an infection or not, given that treatment and outcome are very different, with a 55.3% mortality rate in EG and 29.4% in GE.5
Ethical disclosuresThe authors declare that informed consent was obtained for the publication of the present article. No intervention was performed, complying with the current bioethical research norm. Authorization from the bioethics committee was obtained, explaining that no personal information that could identity the patient appears in the present article.
Financial disclosureNo financial support was received in relation to this article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Pastor-Sifuentes FU, Moctezuma-Velázquez P, Aguilar-Frasco J. Neumatosis gástrica: espectro de la enfermedad. Revista de Gastroenterología de México. 2020;85:219–220.

