

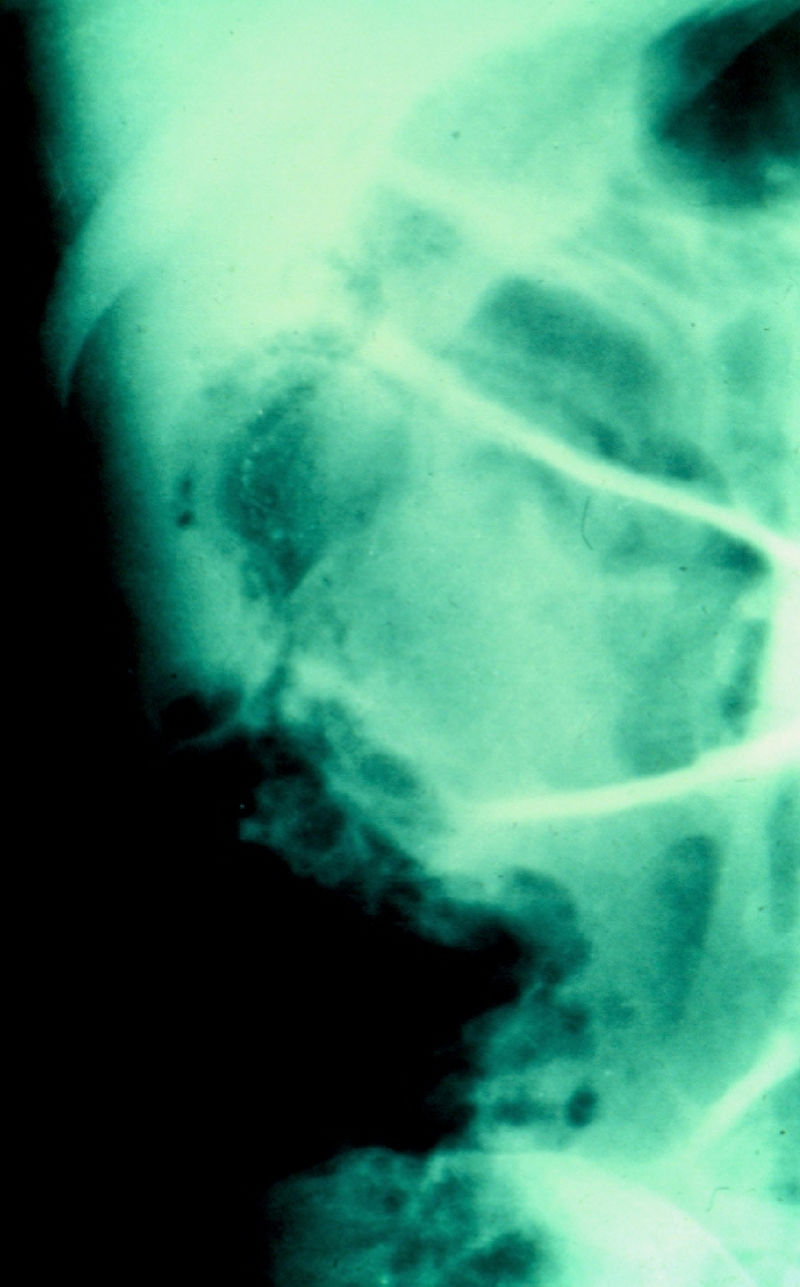

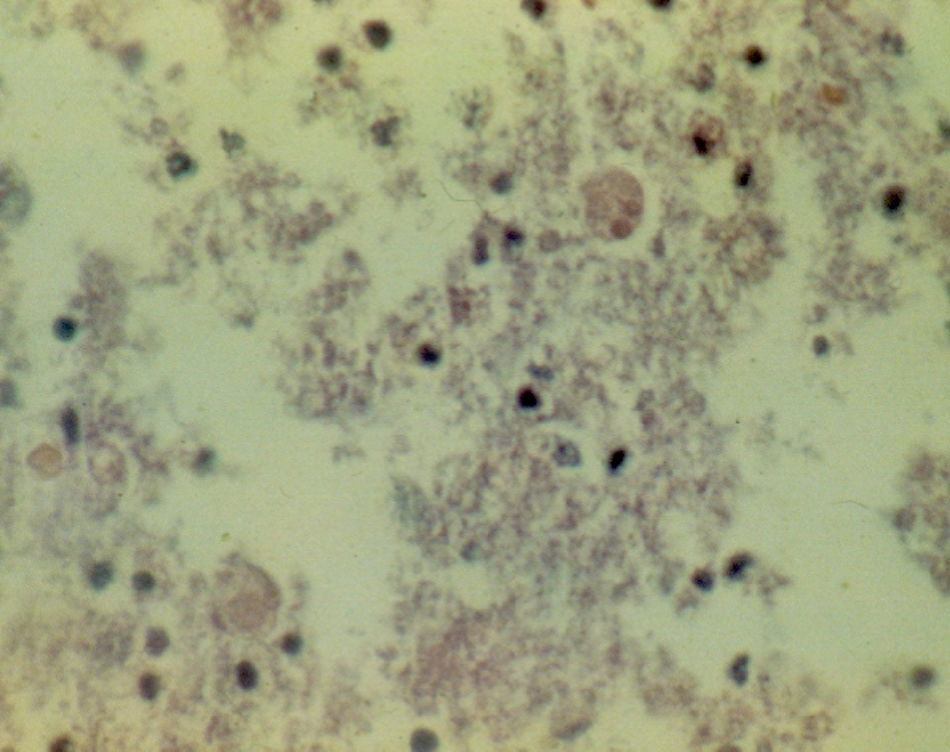
A 67-year-old man had a history of type 2 diabetes mellitus. He sought medical attention for the 7-day progression of 6 to 7 diarrheic stools with mucus and blood per day, fever, nausea, and vomiting of stomach content. He presented with stabbing abdominal pain the last 3 days that began in the lower right quadrant and then became generalized. Physical examination revealed tachycardia, tachypnea, and hyperthermia of 38.7° C. He had acute abdomen with muscle resistance, a positive Blumberg's sign, and reduced peristalsis. Laboratory test results showed leukocytosis, neutrophilia, and bandemia. Plain abdominal x-rays in the standing and decubitus positions identified bowel segment distension and pneumatosis of the wall of the cecum (figs. 1 and 2). Laparotomy revealed areas of necrosis in the entire colon, with fibrinopurulent secretion and crepitation in the cecum. Subtotal colectomy was performed (fig. 3). Indirect hemagglutionation and PCR testing supported the diagnosis of invasive amoebiasis. The histopathology study reported hematophagous trophozoites of Entamoeba histolytica in the wall of the colon1,2 and lymphoplasmacytic infiltrate (fig. 4).




The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of dataThe authors declare that no patient data appear in this article.
Right to privacy and informed consentThe authors declare that no patient data appear in this article.
Financial disclosureNo financial support was received in relation to this study/article.
Conflict of interestThe authors declare that there is no conflict of interest.
Please cite this article as: Rodríguez-Wong U, Rodríguez-Medina U. Colitis amibiana fulminante con neumatosis cecal. Revista de Gastroenterología de México. 2018;83:453–454.

